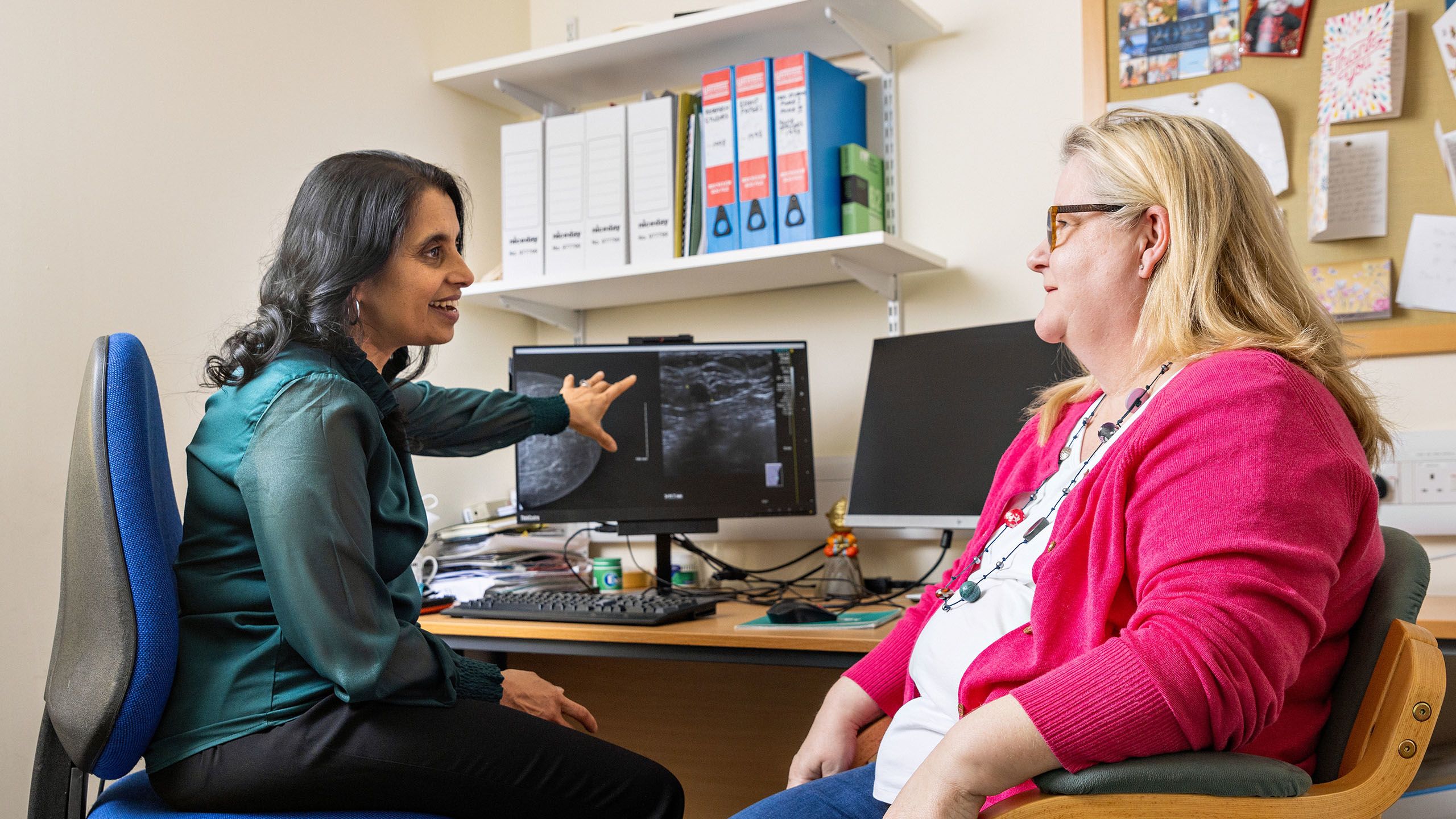
A study involving 900 students in 6 countries found that a short programme of empathy lessons led to measurable, positive changes in their conduct, emotional awareness and curiosity about different cultures.
An analysis of a short programme teaching empathy in schools has found it had a positive impact on students’ behaviour and increased their emotional literacy within 10 weeks.
The findings come from an evaluation of the ‘Empathy Programme‘: a term-long course developed by the UK-based Empathy Studios. The research was conducted with support from academics at the Faculty of Education, University of Cambridge.
Empathy Studios develops school-based, video-led programmes which aim to increase empathy in students aged 5 to 18. Students are shown thought-provoking films, then engage in approximately 30 minutes of activities and discussions about the issues raised. An annual flagship festival of films, resources and events, ‘Empathy Week’, is made available for free and has to date reached 1.3 million students worldwide.
Survey and interview data from 900 students and teachers at 10 participating schools in 6 countries, including the UK, revealed measurable, positive changes in students’ conduct, emotional awareness and curiosity about different cultures and the wider world.
Teachers rated students’ empathy, behaviour and other characteristics on a scale of one to 10 before the programme began, and 5 and 10 weeks later. The average empathy score rose from 5.55 to 7, while average behaviour scores increased from 6.52 to 7.89.
In follow-up interviews, one primary school teacher reflected: “I’ve definitely been able to resolve more issues within the classroom and not have parents called in.” A student told the interviewers: “I think that everyone in the class has become kinder.”
Empathy Studios defines empathy as: “the skill to understand others and the ability to create space for someone to reveal their authentic self while reserving judgement.” The company was founded 4 years ago by Ed Kirwan, a former science teacher from North London.
“The programme’s success lies in teaching students to celebrate difference, which changes their wellbeing and behaviour,” he said. “There’s never an excuse for poor behaviour, but often a reason, which greater mutual understanding can potentially address.”
“I think the social unrest we have seen in Britain this summer shows how urgently we need more empathy across society. It won’t solve everything, but it is the foundation for solutions, and it starts with education. If the new government is serious about curriculum reforms that prepare young people for life and work, we must ensure that school equips them to understand, be curious about, and listen to each other, even in moments of disagreement.”
The evaluation was supported by Dr Helen Demetriou, a specialist in empathy education at the University of Cambridge, who helped to design the research, and to collect, quality assure and interpret the data.
“The findings show that a fairly simple, film-based programme can raise pupils’ empathy levels, enhancing their understanding of themselves, others, and global issues,” she said. “That supports a more complete learning experience, developing social and emotional skills that we know contribute to improved behaviour and more engaged learning.”
Although it is often considered innate, evidence suggests that empathy can be taught. A 2021 study co-authored by Demetriou successfully trialled teaching empathy during design and technology lessons. More recently, researchers at the University of Virginia found that empathy between parents and children is ‘paid forward’ by the children to friends and, later, when they become parents themselves.
Empathy has been linked to better leadership and inclusion in workplaces; while a 2023 World Economic Forum White Paper highlighted the importance of socio-emotional skills to the future of work and argued for more education that emphasises interpersonal skills, including empathy.
Empathy Studios offers schools assembly and lesson plans built around films about the real-life stories of diverse people in other parts of the world. Its 2024/5 programme, for example, profiles 5 individuals from Mexico, including a Paralympian, a dancer, and a women’s rights activist.
Their framework focuses on 3 core concepts: ‘Empathy for Myself’, which develops students’ emotional literacy; ‘Empathy for Others’, which covers mutual understanding and interpersonal relations, and ‘Empathy in Action’, during which the students develop their own social action projects.
The new research builds on a 2022 pilot study with the University of Cambridge, which suggested that the programme makes students more responsive to each others’ feelings and improves self-esteem. The new evaluation involved over 900 students and 30 teachers, and took place during 2023.
The teacher surveys indicated that behaviour had improved by up to 10% in some schools, especially those new to empathy lessons. The average improvement in behaviour recorded by UK teachers corresponded to the overall trend, rising from 6.3/10 pre-programme to 7.7/10 post-programme. Empathy and behaviour also appeared to be closely linked: all schools reporting an overall improvement in student empathy also saw improvements in behaviour after five weeks, which was sustained in 80% of cases after 10.
The evaluation recorded small improvements in students’ overall emotional literacy and their ‘affective empathy’; or their ability to share the feelings of others. A change that emerged strongly from interviews with teachers was that the Empathy Programme appeared to increase students’ interest in other cultures. In one primary school, for example, the proportion of students responding positively to the statement “I want to find out more about the world” rose from 86% to 96% after 10 weeks. This echoes Organisation for Economic Co-operation and Development (OECD) evidence linking empathy to civic engagement.
Many students said they had learned valuable lessons from the programme. Their reflections included: “Everyone struggles… I’m not the only one who finds it hard”, and “Although we are all different, we all have so much in common”.
“Empathy is the number one human skill we need to develop for the future,” Kirwan said. “It should not just be an add-on; it should be considered foundational.”
Major milestone for first specialist children’s hospital in the East of England.
Plans for Cambridge Children’s Hospital can move ahead following the news that the Outline Business Case for the project has been signed off by the Chief Secretary to the Treasury and the Secretary of State for Health and Social Care. The project has been given the green light to begin the detailed process of appointing a contractor, to build the ground-breaking new facility in 2026.
The ministerial backing means that the Project’s Outline Business Case, the second stage of the business case process, has now been fully approved by the Department of Health and Social Care, NHS England and HM Treasury. It was approved in principle in September 2023, subject to a capital affordability review by NHS England and the Department for Health and Social Care’s Joint Investment Committee. That review took place in April 2024 and resulted in a recommendation to Ministers to endorse the decision.
In a show of further confidence in its plans, the Outline Business Case was signed off by the Chief Secretary to the Treasury and the Secretary of State for Health and Social Care in August 2024. This approval recognises that the hospital will meet the needs of patients and staff across the East of England and that the project has the appropriate funding streams in place, to deliver the specialist children’s facility.
The hospital is being co-designed with the help of children, young people, families and healthcare professionals across the region to ensure the new hospital will meet the needs of patients, families and staff.
Dr Rob Heuschkel, Clinical Lead for Physical Health at Cambridge Children’s Hospital said:
“We are absolutely delighted that we can now move forward to enter contracts with a construction partner, so we can finally start to see work happening on site.
“A huge amount of work has gone into finalising the designs and getting us to this point, and I want to thank our healthcare staff, young people and their families from across the region who have been contributing valuable feedback and helping us shape our plans, right from the very start.
“The East of England is the only region in the UK without a specialist children’s hospital, and we look forward to changing that very soon.”
The approval comes as a programme of groundworks preparing for the build was completed in July, and new access roads have now been installed where the new five-storey, 35,000sqm hospital will be located, opposite the Rosie Maternity Hospital, on Robinson Way and Dame Mary Archer Way.
In the coming weeks, people will be able to see hoardings installed around the site of Cambridge Children’s Hospital, the first hospital truly designed to bring mental and physical health care together for children and young people.
Dr Isobel Heyman, Clinical Lead for Mental Health at Cambridge Children’s Hospital said:
“This really is fantastic news and an exciting moment in our journey to build a truly integrated children’s hospital for the East of England.
“The current model of mental health care is inadequate. Many children with physical ill-health also have significant mental health needs, and vice versa.
“Cambridge Children’s Hospital offers a solution. By delivering holistic care for children, young people, and their families, this not only reduces stigma, but the revolutionary model of care really does act as a blueprint for the NHS and the future of healthcare.”
The fundraising Campaign for Cambridge Children’s Hospital has now passed the halfway mark and the project remains on track to meet its £100m philanthropy target.
The hospital will also house a University of Cambridge research institute, focused on preventing childhood illness and early intervention across mental and physical healthcare.
Professor David Rowitch, Clinical Lead for Research at Cambridge Children’s Hospital said:
“By bringing clinicians and patients together with University of Cambridge investigators and industry partners, we aim to shift the medicine paradigm from traditional reactive approaches, to one based on early detection, precision intervention and disease prevention.
“Co-locating research efforts inside Cambridge Children’s Hospital will mean we can detect disease early or even prevent it altogether, personalise health care and prescribe treatments more appropriate for children and their individual health needs.
“We’ll also be able to foster collaborations to advance the power of advanced diagnostics, digital and telehealth technology to support healthcare professions from a distance, to deliver care closer to people’s homes, wherever they live in our region.”
The Cambridge Children’s Hospital project is a partnership between Cambridge University Hospitals NHS Foundation Trust (CUH), Cambridgeshire and Peterborough NHS Foundation Trust (CPFT), and the University of Cambridge.
Work now continues on the final stage of the business case for Cambridge Children’s Hospital – the Full Business Case.
Researchers have discovered a way to extend the shelf life of blood stem cells outside the body for use in gene therapy, providing patients with better options and improving their outcomes.
We were able to identify a key molecular pathway…that can be targeted by a drug which is already in use and is safe to use.Elisa Laurenti
Researchers have identified a drug already used for cancer patients, that, when applied to current gene therapy protocols can improve blood stem cell function threefold.
One trillion blood cells are produced every day in humans, and blood stem cells are the only cell types in our body capable of producing all blood cell types over our lifespan, giving them immense regenerative potential.
Blood stem cell gene therapy is a ground-breaking treatment that currently provides the only cure to more than ten life-debilitating genetic diseases and has already saved the lives of more than two million people with blood cancers and other diseases.
These therapies take blood stem cell samples from patients, where their genetic defect is corrected in a dish before being delivered back to the patient. However, limitations persist in blood stem cell therapies because of the shelf life of the cells outside the body. When removed from their environment in the human body and cultured in a dish, most blood stem cells lose their function. The exact timing and cause of this function loss has not previously been well understood.
Now, scientists in the Laurenti Group and others at the University of Cambridge’s Cambridge Stem Cell Institute (CSCI) and Department of Haematology have pinpointed a timeline for the blood stem cells under the current gene therapy protocols, which typically take place over three days. After the first 24 hours in a dish, more than 50% of the blood stem cells can no longer sustain life-long blood production, which is before therapy would even begin in a clinical setting.
During those first 24 hours, the cells activate a complex molecular stress response in order to adapt to the dish. By studying this stress response, the team identified a solution. Through repurposing a cancer growth blocker drug (Ruxolitinib), already in use for cancer treatments, they were able to improve stem cell function in a dish by three times its former capabilities.
The group is now aiming to modify current gene therapy protocols to include this drug, providing patients with the highest number of high-quality blood stem cells and improving their outcomes.
Professor Elisa Laurenti at the University of Cambridge Stem Cell Institute, and senior author of the study, said: “This is really exciting because we are now in a position where we can begin to understand the huge stress that these stem cells sense when they are manipulated outside of our body. Biologically it is really fascinating because it affects every aspect of their biology. Luckily, we were able to identify a key molecular pathway which governs many of these responses, and that can be targeted by a drug which is already in use and is safe to use.
“I hope our findings will enable safer treatments for gene therapy patients. Our discovery also opens up many possibilities to better expand blood stem cells ex vivo and expand the set of disease where we can use blood stem cells to improve patients’ lives.”
Dr Carys Johnson at the University of Cambridge Stem Cell Institute, and first author of the study, said: “Although we expected that removing these cells from the body and culturing them on a plastic surface would alter gene expression, the extent of change we found was surprising, with over 10,000 genes altered and a significant stress response detected. It was also striking to discover that the majority of blood stem cells are functionally lost during gene therapy protocols, before transplantation back to the patient.
“We have identified a key bottleneck where function is lost and clinical culture could be improved. I hope that our work will drive advancements in culture protocols to better harness the power of blood stem cells and improve the safety and efficacy of clinical approaches.”
Around one in four patients with severe brain injury who cannot move or speak – because they are in a prolonged coma, vegetative or minimally conscious state – is still able to perform complex mental tasks, a major international study has concluded in confirmation of much smaller previous studies.
When a patient has sustained a severe brain injury, there are very important, and often difficult, decisions to be made by doctors and family members about their careEmmanuel Stamatakis
Severe brain injury can leave individuals unable to respond to commands physically, but in some cases they are still able to activate areas of the brain that would ordinarily play a role in movement. This phenomenon is known as ‘cognitive motor dissociation’.
To determine what proportion of patients in so-called ‘disorders of consciousness’ experience this phenomenon – and help inform clinical practice – researchers across Europe and North America recruited a total of 353 adults with disorders of consciousness, including the largest cohort of 100 patients studied at Cambridge University Hospitals NHS Foundation Trust.
Participants had mostly sustained brain injury from severe trauma, strokes or interrupted oxygen supply to the brain after heart attacks. Most were living in specialised long-term care facilities and a few were living at home with extensive care packages. The median time from injury for the whole group was about eight months.
Researchers assessed patterns of brain activation among these patients using functional magnetic resonance imaging (fMRI) or electroencephalography (EEG). Subjects were asked to repeatedly imagine performing a motor activity (for example, “keep wiggling your toes”, “swinging your arm as if playing tennis”, “walking around your house from room to room”) for periods of 15 to 30 seconds separated by equal periods of rest. To be able to follow such instructions requires not only the understanding of and response to a simple spoken command, but also more complex thought processes including paying attention and remembering the command.
The results of the study are published today in the New England Journal of Medicine.
Dr Emmanuel Stamatakis from the Department of Clinical Neurosciences at the University of Cambridge said: “When a patient has sustained a severe brain injury, there are very important, and often difficult, decisions to be made by doctors and family members about their care. It’s vitally important that we are able to understand the extent to which their cognitive processes are still functioning by utilising all available technology.”
Among the 241 patients with a prolonged disorder of consciousness, who could not make any visible responses to bedside commands, one in four (25%) was able to perform cognitive tasks, producing the same patterns of brain activity recorded with EEG and/or fMRI that are seen in healthy subjects in response to the same instructions.
In the 112 patients who did demonstrate some motor responses to spoken commands at the bedside, 38% performed these complex cognitive tasks during fMRI or EEG. However, the majority of these patients (62%) did not demonstrate such brain activation. This counter-intuitive finding emphasises that the fMRI and EEG tasks require patients to have complex cognitive abilities such as short-term memory and sustained concentration, which are not required to the same extent for following bedside commands.
These findings are clinically very important for the assessment and management of the estimated 1,000 to 8,000 individuals in the UK in the vegetative state and 20,000 to 50,000 in a minimally conscious state. The detection of cognitive motor dissociation has been associated with more rapid recovery and better outcomes one year post injury, although the majority of such patients will remain significantly disabled, albeit with some making remarkable recoveries.
Dr Judith Allanson, Consultant in Neurorehabilitation, said: “A quarter of the patients who have been diagnosed as in a vegetative or minimally conscious state after detailed behavioural assessments by experienced clinicians, have been found to be able to imagine carrying out complex activities when specifically asked to, is sobering. This sobering fact suggests that some seemingly unconscious patients may be aware and possibly capable of significant participation in rehabilitation and communication with the support of appropriate technology.
“Just knowing that a patient has this ability to respond cognitively is a game changer in terms of the degree of engagement of caregivers and family members, referrals for specialist rehabilitation and best interest discussions about the continuation of life sustaining treatments.”
The researchers caution that care must be taken to ensure the findings are not misrepresented, pointing out, for example, that a negative fMRI/EEG result does not per se exclude cognitive motor dissociation as even some healthy volunteers do not show these responses.
Professor John Pickard, emeritus professorial Fellow of St Catharine’s College, Cambridge, said: “Only positive results – in other words, where patients are able to perform complex cognitive processes – should be used to inform management of patients, which will require meticulous follow up involving specialist rehabilitation services.”
The team is calling for a network of research platforms to be established in the UK to enable multicentre studies to examine mechanisms of recovery, develop easier methods of assessment than task-based fMRI/EEG, and to design novel interventions to enhance recovery including drugs, brain stimulation and brain-computer interfaces.
The research reported here was primarily funded by the James S. McDonnell Foundation. The work in Cambridge was supported by the National Institute for Health and Care Research UK, MRC, Smith’s Charity, Evelyn Trust, CLAHRC ARC fellowship and the Stephen Erskine Fellowship (Queens’ College).
Reference Bodien, YG et al. Cognitive Motor Dissociation in Disorders of Consciousness. NEJM; 14 Aug 2024; DOI: 10.1056/NEJMoa2400645
Adapted from a press release from Weill Cornell Medicine
Acknowledgements
The multidisciplinary Cambridge Impaired Consciousness Research Group, led by Emeritus Professors John Pickard (Neurosurgery) & David Menon (Anaesthesia) and Drs Judith Allanson & Emmanuel A. Stamatakis (Lead, Cognition and Consciousness Imaging Group), started its research programme in 1997, partly in response to emerging concern over the misdiagnosis of the vegetative state. This pioneering work has only been possible by having access to the world class resources of the Wolfson Brain Imaging Centre, the NIHR/Wellcome Clinical Research Facility at Addenbrooke’s Hospital, the MRC Cognition and Brain Sciences Unit (Professors Barbara Wilson & Adrian Owen), the Royal Hospital for Neuro-disability (Putney) and the Central England Rehabilitation Unit (Royal Leamington Spa).
Pollutants preserved in Antarctic ice document historic fires in the Southern Hemisphere, offering a glimpse at how humans have impacted the landscape and providing data that could help scientists understand future climate change.
Researchers from the University of Cambridge and the British Antarctic Survey tracked fire activity over the past 150 years by measuring carbon monoxide trapped in Antarctic ice. This gas is released, along with smoke and particulates, by wildfires, cooking and communal fires.
The findings, reported in the Proceedings of the National Academy of Sciences, reveal that biomass burning has been more variable since the 1800s than had been thought. The new data could help improve climate models, which rely on information about past atmospheric gases, such as carbon monoxide, to improve their forecasts.
“We’ve been missing key information from the period when humans started to dramatically alter Earth’s climate; information needed to test and develop climate models,” said Rachael Rhodes, senior author of the paper from Cambridge’s Department of Earth Sciences.
The new carbon monoxide record fills that gap in time. The researchers charted the strength of biomass burning between 1821 and 1995 by measuring carbon monoxide in ice cores from Antarctica. The layers of ice inside these cores formed when snow was buried under subsequent years’ snowfall, encasing pockets of air that directly sample the atmosphere’s composition at the time.
“It’s rare to find trace gases trapped in ice cores for the most recent decades,” said Ivo Strawson, lead author of the study who is jointly based at Cambridge Earth Sciences and the British Antarctic Survey. “We need information on the atmosphere’s composition following the onset of industrialisation to reduce uncertainties in climate models, which rely on these records to test or drive their simulations.”
A major difficulty with taking gas measurements from very young ice is that pressurised air bubbles haven’t had time to form under the weight of more snow, said Strawson. To get around this problem, the researchers studied ice from locations where snow accumulates rapidly. These ice cores, held in BAS’ dedicated Ice Core Laboratory, were collected from the Antarctic Peninsula as part of previous international projects.
To measure carbon monoxide, the researchers developed a state-of-the-art analysis method, which melts ice continuously while simultaneously extracting the air. They collected tens of thousands of gas measurements for the past 150 years.
The researchers found that the strength of biomass burning has dropped steadily since the 1920s. That decline, said Rhodes, coincides with the expansion and intensification of agriculture in southern Africa, South America, and Australia during the early 20th century. With wildlands converted into farmland, forest cover was restricted and in turn fire activity dropped. “This trend reflects how land conversion and human expansion have negatively impacted landscapes and ecosystems, causing a major shift in the natural fire regime and in turn altering our planet’s carbon cycle,” said Rhodes.
One assumption made by many climate models, including those used by the IPCC, is that fire activity has increased in tandem with population growth. But, said Rhodes, “our work adds to a growing mass of evidence that this assumption is wrong, and the inventories of historic fire activity need to be corrected so that models can accurately replicate the variability we see in our record.”
Rachael Rhodes is a Fellow of Wolfson College, Cambridge.
Offering patients with concussion a type of brain scan known as diffusion tensor imaging MRI could help identify the one in three people who will experience persistent symptoms that can be life changing, say Cambridge researchers.
Concussion is the number one neurological condition to affect adults, which is why we need a way of identifying those patients at greatest risk of persistent symptomsVirginia Newcombe
Around one in 200 people in Europe every year will suffer concussion. In the UK, more than 1 million people attend Emergency Departments annually with a recent head injury. It is the most common form of brain injury worldwide.
When a patient in the UK presents at an Emergency Department with head injury, they are assessed according to the NICE head injury guidelines. Depending on their symptoms, they may be referred for a CT scan, which looks for brain injuries including bruising, bleeding and swelling.
However, CT scans identify abnormalities in fewer than one in 10 patients with concussion, yet 30-40% of patients discharged from the Emergency Department following a scan experience significant symptoms that can last for years and be potentially life-changing. These include severe fatigue, poor memory, headaches, and mental health issues (including anxiety, depression, and post-traumatic stress).
Dr Virginia Newcombe from the Department of Medicine at the University of Cambridge and an Intensive Care Medicine and Emergency Physician at Addenbrooke’s Hospital, Cambridge, said: “The majority of head injury patients are sent home with a piece of paper telling them the symptoms of post-concussion to look out for and are told to seek help from their GP if their symptoms worsen.
“The problem is that the nature of concussion means patients and their GPs often don’t recognise that their symptoms are serious enough to need follow-up. Patients describe it as a ‘hidden disease’, unlike, say, breaking a bone. Without objective evidence of a brain injury, such as a scan, these patients often feel that their symptoms are dismissed or ignored when they seek help.”
In a study published today in eClinicalMedicine, Dr Newcombe and colleagues show that an advanced form of MRI known as diffusion tensor imaging (DTI) can substantially improve existing prognostic models for patients with concussion who have been given a normal CT brain.
DTI measures how water molecules move in tissue, providing detailed images of the pathways, known as white matter tracts, that connect different parts of the brain. Standard MRI scanners can be adapted to measure this data, which can be used to calculate a DTI ‘score’ based on the number of different brain regions with abnormalities.
Dr Newcombe and colleagues studied data from more than 1,000 patients recruited to the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) study between December 2014 and December 2017. 38% of the patients had an incomplete recovery, meaning that three months after discharge their symptoms were still persisting.
The team assigned DTI scores to the 153 patients who had received a DTI scan. This significantly improved the accuracy of the prognosis – whereas the current clinical model would correctly predict in 69 cases out of 100 that a patient would have a poorer outcome, DTI increased this to 82 cases out of 100.
Whole brain diffusion tensor tractography showing healthy patient (left) and patient at two days (centre) and six weeks (right) after severe traumatic brain injury (Credit: Virginia Newcombe)
The researchers also looked at blood biomarkers – proteins released into the blood as a result of head injury – to see whether any of these could improve the accuracy of the prognosis. Although the biomarkers alone were not sufficient, concentrations of two particular proteins – glial fibrillary acidic protein (GFAP) within the first 12 hours and neurofilament light (NFL) between 12 and 24 hours following injury – were useful in identifying those patients who might benefit from a DTI scan.
Dr Newcombe said: “Concussion is the number one neurological condition to affect adults, but health services don’t have the resources to routinely bring back every patient for a follow-up, which is why we need a way of identifying those patients at greatest risk of persistent symptoms.
“Current methods for assessing an individual’s outlook following head injury are not good enough, but using DTI – which, in theory, should be possible for any centre with an MRI scanner – can help us make much more accurate assessments. Given that symptoms of concussion can have a significant impact on an individual’s life, this is urgently needed.”
The team plan to look in greater details at blood biomarkers, to see if they can identify new ways to provide even simpler, more practical predictors. They will also be exploring ways to bring DTI into clinical practice.
Dr Sophie Richter, a NIHR Clinical Lecturer in Emergency Medicine and first author, Cambridge, added: “We want to see if there is a way to integrate the different types of information obtained when a patient presents at hospital with brain injury – symptoms assessment, blood tests and brain scans, for example – to improve our assessment of a patient’s injury and prognosis.”
The research was funded by European Union’s Seventh Framework Programme, Wellcome and the National Institute for Health and Care Excellence.
Cambridge researchers have cast doubt on whether new amyloid immunotherapy drugs will have the desired effect of significantly reducing the impact of Alzheimer’s disease.
While the current amyloid immunotherapies may show a glint of promise for very selected groups, it’s clear these drugs will not address dementia risk at scaleCarol Brayne
Writing in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association, the team from Cambridge Public Health argue that substantial challenges including the risk-benefit ratio, limited eligibility and high cost of roll-out will limit any benefits of these treatments.
Alzheimer’s disease is often quoted as causing 70% of the 55 million cases of dementia worldwide, though the definition of what constitutes the disease is hotly debated. One characteristic of Alzheimer’s is the build-up of clusters of misfolded proteins, one of these being a form of amyloid, leading to plaques in the brain. The cascade hypothesis, a dominant theory in the field, suggests that this triggers a series of processes which together lead to dementia symptoms.
Advances in developing treatments to reduce symptoms and slow down the progression in the early stages of Alzheimer’s has been slow. However, there has been recent excitement surrounding amyloid immunotherapy agents, drugs that harness the immune system to remove amyloid pathology.
Two completed phase III randomised controlled trials of amyloid immunotherapy reported statistically significant reductions in the rate of cognitive and functional decline compared to the placebo.
But as the Cambridge team point out, the effect sizes were small – small enough that a doctor would struggle to tell the difference between the average decline of a patient on the drug and another on placebo, after 18 months. The drugs were also associated with significant adverse events, including brain swelling and bleeding; during the phase III trial of one agent, donanemab, there were also three deaths attributed to the treatment.
Crucially, there is little known about the long-term effects of the drugs beyond the 18 month trial periods. Long-term placebo-controlled trials, which would be needed to see if there is any clinically meaningful slowing of decline, are unlikely to be feasible where drugs are already approved.
Despite this, the US Food and Drug Administration has licensed two such drugs. The European Medicines Agency (EMA) has recommended rejecting one (lecanemab) predominantly on the grounds that the small effects seen do not outweigh the risk from side effects; it is reviewing the other. The UK’s Medicines and Healthcare Products Regulatory Agency (MHRA) is expected to take a decision on both drugs imminently.
Edo Richard, Professor of Neurology at Radboud University Medical Centre in Nijmegen, The Netherlands, and co-author, said: “If these drugs are approved by regulators in the UK and Europe, and become available, it is understandable that some people with early Alzheimer’s will still want to try these drugs, given their despair living with this dreadful disease. But there is a lot of hyperbole around the reporting of these drugs, and significant effort will be needed to provide balanced information to patients to enable informed decisions.”
Press coverage of the drugs has implied they are suitable for anyone with a diagnosis of Alzheimer’s. However, while the trials included those with ‘early symptomatic Alzheimer’s disease’, it excluded those with other conditions that may have been contributing to their symptoms. Evidence suggests that the people in the trials represent less than 8% of those in the community with early Alzheimer’s disease. Those in the trials were up to 10 to 15 years younger than those typically presenting to health services with early symptoms.
Lead author Dr Sebastian Walsh, NIHR Doctoral Fellow in Public Health Medicine at Cambridge Public Health, University of Cambridge, added: “If approved, the drugs are likely to be relevant only for a relatively small cohort of Alzheimer’s patients, so potential recipients will need to undergo a range of assessments before being given access to the drugs. Plus, effect sizes seen in the trials are very small and the drugs will need be administered as early in the disease process as possible, when symptoms are mild – and people in these phases of disease can be hard to identify.”
The resource requirements for rolling out such treatments are likely to be considerable. Even if approved for only a small proportion of Alzheimer’s patients, a much broader group of people will need to be assessed for eligibility, requiring rapid specialist clinical assessment and tests. The authors question whether this is the best use of these resources, given the strain health systems are already under. Support would also be required for the large number of Alzheimer’s patients (potentially as many as 92%) found to be ineligible. Those found to have insufficient amyloid to be eligible may then require follow-up assessments to determine eligibility in the future, with the further implications for services this would entail.
Professor Carol Brayne, Co-director of Cambridge Public Health, said: “Even in high-income countries, rolling out such types of treatments at scale is highly challenging, but most dementia occurs in low- and middle-income countries. Health systems in these countries are highly unlikely to have the resources required to offer these new drugs, even to a very narrow group.
“Other compelling evidence suggests that attention to inequalities and health experience across people’s lives could have greater impact on the rates of dementia in populations. Most dementia is more complicated than a single protein.”
The team concludes that based on current evidence, it is far from clear whether amyloid immunotherapy can ever significantly reduce suffering caused by dementia at scale in the community, and we must continue to explore other approaches.
Professor Brayne added: “With an ageing population, we urgently need effective ways to support people living with dementia, but while the current amyloid immunotherapies may show a glint of promise for very selected groups, it’s clear these drugs will not address dementia risk at scale.”
To protect the Amazon and support the wellbeing of its people, its economy needs to shift from environmentally harmful production to a model built around the diversity of indigenous and rural communities, and standing forests.
A group of conservationists from Bolivia, Brazil, Peru, Ecuador, the US and the UK say that current conservation and development efforts will never sustain or scale without systemic changes in how economies are designed.
Despite extensive destruction of the Amazon in the name of economic development, Amazonian communities have seen little improvement in income, life expectancy, and education. The researchers have proposed a new model and associated policy changes that could create fair and sustainable futures for the Amazon and its people by improving infrastructure, supply chains, and social organisations.
Their results, reported in the journal Nature Ecology and Evolution, are focused on the Amazon, however the researchers say similar economic models could be implemented around the world if the political will exists.
The Amazon basin is home to the world’s largest tropical rainforest, representing over half of the world’s remaining rainforest, and stores vast amounts of carbon. However, decades of large-scale deforestation, as well as the increased risk of fires and floods due to climate change, has put much of the Amazon rainforest under threat. In addition to what the loss of the Amazon would mean for global carbon emissions, the rainforest is also home to many indigenous peoples and thousands of species of plants and animals.
“We need a different vision for the Amazon if we’re going to protect it,” said lead author Professor Rachael Garrett from the University of Cambridge’s Department of Geography and the Conservation Research Institute. “Half a century of deforestation and exploitation of the Amazon has not resulted in widespread development, and now the economic value of deforested areas is threatened, not to mention the threats to the global climate and water security.”
Working with colleagues from the Amazonian region, Garrett has proposed building on the success of indigenous and traditional communities to develop new economies, which could protect much of the Amazon while also improving the livelihoods, health, and food security of the many people who live there. These economic models are known as socio-bioeconomies, or SBEs.
“Conventional economic models can result in short-term gains, but over the longer term, the people and resources of the Amazon basin have been exploited by powerful interests, while there has been an underinvestment in education, innovation, and sustainable infrastructure,” said Garrett. “The conventional economic model is simply not sustainable.”
The SBE model is focused on using and restoring Amazonian and other ecosystems sustainably, and supporting indigenous and rural communities. An SBE economy might include eco-friendly tourism, or the sustainable harvest and processing of plant products into valuable foods, beverages, clothing, and medicines.
“A limited range of interests are controlling the development agenda in most countries,” said Garrett. “The only way we can change that is improving the rights and representation of the people who are not benefiting from the systems and are being harmed by ongoing environmental destruction. We believe it is possible to have win-wins for humanity and conservation, but not if we continue to consume products that have a massively negative impact. SBEs can help put these win-wins into policy and practice.”
Garrett cites the footwear brand Veja as an example of such a win-win. The French company buys the rubber for its trainers from small-scale Amazonian rubber farmers, and purchases 100% of the responsibly harvested native rubber in Brazil. As part of its sustainability efforts, the company focuses on building communities of small-scale farmers and has been financially successful without traditional advertising.
Garrett and her collaborators are calling for massive increases in social mobilisation, technology and infrastructure to support SBEs. Under an SBE model, governmental subsidies would be redirected away from agribusiness and toward smaller-scale sustainable development. The researchers also outline how to build connections between rural and urban policies in SBEs. An example is the establishment of public procurement programmes where healthy and sustainably produced foods are purchased directly from indigenous and small farming communities and served in school lunch programmes and hospitals, instead of supporting large-scale agribusiness engaged in degrading practices.
Other policy changes that could support an SBE model include redirecting finance to conservation and restoration activities, supporting community enterprises, and ensuring participatory processes to ensure inclusive, long-term benefits.
“It’s possible to have an economy that is strong and works for everyone when we dare to develop new models and visions that recognise the interconnectedness of people and nature,” said Garrett. “By popularising these ideas, investing in people and businesses who are making a difference, and supporting research into SBE innovation we can support a transformation in both conservation and development in the Amazon.
“The SBE model could help protect the Amazon and its people while avoiding climate and biodiversity disasters, but there needs to be the political will to make it happen.”
Rachael Garrett is the incoming director of the University of Cambridge Conservation Research Institute and a Fellow of Homerton College, Cambridge. She is a council member of the Cambridge Conservation Initiative and serves on the UN Science Panel for the Amazon.
Astronomers have discovered that red dwarf stars can produce stellar flares that carry far-ultraviolet (far-UV) radiation levels much higher than previously believed.
The discovery suggests that the intense UV radiation from these flares could significantly impact whether planets around red dwarf stars can be habitable.
“Few stars have been thought to generate enough UV radiation through flares to impact planet habitability. Our findings show that many more stars may have this capability,” said first author Vera Berger, who led the research while based at the University of Hawai’i and who is now based at the University of Cambridge.
Berger and her team used archival data from the GALEX space telescope to search for flares among 300,000 nearby stars. GALEX is a now-decommissioned NASA mission that simultaneously observed most of the sky at near-and far-UV wavelengths from 2003 to 2013. Using new computational techniques, the team mined insights from the data.
“Combining modern computer power with gigabytes of decades-old observations allowed us to search for flares on thousands and thousands of nearby stars,” said co-author Dr Michael Tucker from Ohio State University.
According to researchers, UV radiation from stellar flares can either erode planetary atmospheres, threatening their potential to support life, or contribute to the formation of RNA building blocks, which are essential for the creation of life.
The study, published in the Monthly Notices of the Royal Astronomical Society, challenges existing models of stellar flares and exoplanet habitability, showing that far-UV emission from flares is on average three times more energetic than typically assumed, and can reach up to twelve times the expected energy levels.
“A change of three is the same as the difference in UV in the summer from Anchorage, Alaska to Honolulu, where unprotected skin can get a sunburn in less than 10 minutes,” said co-author Benjamin J. Shappee from the University of Hawai’i.
The exact cause of this stronger far-UV emission remains unclear. The team believes it might be that flare radiation is concentrated at specific wavelengths, indicating the presence of atoms like carbon and nitrogen.
“This study has changed the picture of the environments around stars less massive than our Sun, which emit very little UV light outside of flares,” said co-author Jason Hinkle.
According to Berger, now a Churchill Scholar at Cambridge, more data from space telescopes is needed to study the UV light from stars, which is crucial for understanding the source of this emission.
“Our work puts a spotlight on the need for further exploration into the effects of stellar flares on exoplanetary environments,” said Berger. “Using space telescopes to obtain UV spectra of stars will be crucial for better understanding the origins of this emission.”
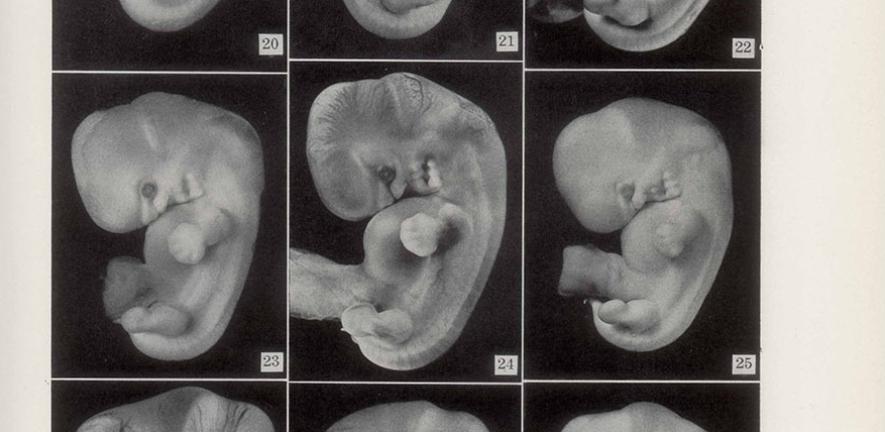
A new study takes a tour of the history of research into human embryology and development to show the “cycles of attention” that led to major scientific breakthroughs.
Analysing the past sheds light on the present resurgence of research on human development. That’s the lesson of a new study by Professor Nick Hopwood, from the Department of History and Philosophy of Science, that is published in the Journal of the History of Biology. The paper discusses the flourishing of human embryology a century ago, its drop in popularity after World War II, and especially its revival since the late twentieth century.
“Every journal article and news story about human development includes a bit of history, but it’s often narrow, rarely informative and not always accurate”, Hopwood says. “I wanted to stand back and see a bigger picture, then dig down to find out how and why there has been such a surge of attention. Working in Cambridge made that easier.”
The University has been at the forefront of innovation, from the first test-tube baby to the extended culture of early embryos, organoids and other stem-cell models. The networking through Cambridge Reproduction of expertise in science and medicine, humanities and social sciences helped Hopwood reconstruct the genesis of these advances. This took a combination of research in libraries and archives and interactions with scientists, including interviews, sharing of documents, attending conferences and giving talks, here and elsewhere.
“Human development has long been of special interest as evidence of our origins and for its medical relevance, but is hard to study”, Hopwood explains. “Historically there have been two main approaches. Either deciding that it’s too difficult to research human embryos because they’re usually hidden in pregnant bodies, so we should study other animals and hope results will transfer. That’s an indirect approach. Or trying for the best possible results from the few human specimens that can be obtained. That’s a direct approach. My article analyses the rise of research directly on human material as part of the changing politics of choosing a species to study. I explore how researchers distanced themselves from work on animal models but even human studies depended on this.”
Interest in human embryos grew in the later 19th century, following debates about evolution. Darwinists pointed to the similarity of humans and other animals at early stages as evidence of common descent. Critical anatomists responded by setting up networks of physicians to collect material, mainly from women’s pregnancy losses. New techniques such as serial sectioning and wax modelling from the slices made details of internal structure visible in 3-D.
This led to a watershed moment: the establishment by the Carnegie Institution of Washington of a Department of Embryology at Johns Hopkins University in Baltimore. Founded in 1914, the first research institution devoted specifically to embryology focused on human embryos, now also increasingly recovered from aseptic operations for various conditions. Important discoveries include elucidation of the timing of ovulation in the menstrual cycle, initially in rhesus macaques. Human embryos from the first two weeks after fertilization were described for the first time.
Flies, frogs and chicks
After World War II human embryology ran out of steam. A new field, developmental biology, focused on model organisms, such as flies, frogs, chicks and, as the exemplary mammal, mice.
“To make progress, the argument went, it was necessary to work on species where more could be done more easily”, Hopwood explains. “That meant micromanipulation, enough material to do biochemistry and molecular biology, and genetic tools.” This approach demonstrated its power in the 1980s, when mechanisms of development were found to be more conserved across the animal kingdom than researchers had imagined. Yet from around the same time interest revived in using human material.
“There was not a steadily rising curve of research on human development through the twentieth century”, Hopwood contends. “Instead, human embryos have gone through cycles of attention and neglect. As opportunities opened up and the balance of power shifted between researchers invested in different organisms, so the politics of species choice have changed. Over the last four decades we’ve seen a renewal of research directly on human development. This is in the first place because of changes in supply and demand.”
The achievement of human in-vitro fertilisation, with a live birth in 1978, gave access to embryos before implantation in the uterus. After much debate the UK Human Fertilisation and Embryology Act 1990 permitted donated embryos to be kept in vitro, under strict regulations, for up to 14 days from fertilization. Though only in 2016 was that limit approached. Meanwhile, biobanks, notably the Human Developmental Biology Resource in Newcastle and London, provided ethical supplies of post-implantation stages from terminations of pregnancy.
There has been opposition from anti-abortion activists, and many fewer embryos are donated for research than scientists (and some patients) would like. But the field was transformed. As in the years around 1900, new technologies eased the study of human embryos. Only now the advances were in digital communication, molecular analysis and imaging methods. Optical slices and computer graphics replaced microscope slides and wax models.
Beyond mice
To obtain human embryos with permission and funding to study them, researchers had to make the case for studying our own species. They stimulated demand by arguing that it would no longer do simply to extrapolate from mice. Knowledge and skills from the mouse model could be applied, but the differences as well as the similarities had to be explored. That was crucial before clinical application, as in fertility treatments. It was also desirable in discovering what makes us human—or at least not mice. Funders were keen to support medically relevant research or “translational science”.
In the last fifteen years another kind of model has transformed the politics of species choice. Subject to ongoing ethical negotiations, stem-cell-based embryo models have enabled fresh kinds of experiment on human development. Some researchers even argue that, for investigating fundamentals of vertebrate development, these human systems are now the model. Mice remain a crucial resource, with almost every innovation made on them first. But since their development is rather peculiar, other laboratories are promoting comparisons with species that develop more like humans.
Around ten years ago, all this inspired the organization of a new sub-field, human developmental biology, not least through a series of conferences. Major research programmes, such as the Human Developmental Biology Initiative, bring together scientists working, in different ways, on various aspects of embryogenesis.
Questions remain. Hopwood’s historical research concentrated on the USA and the UK, with nods to continental Europe and Japan. It would be good to explore other countries’ histories, he suggests, especially since differences in reproductive politics and infrastructure mean that access to material is uneven.
More generally, Hopwood argues, “history can contribute by showing how we got here and clarifying the arguments that have been used”. “It helps stakeholders see why there are now such opportunities for research on human development, and that, because arrangements are fragile, it will take work to gain and keep public support.” So a long-term perspective can assist researchers and funders in thinking about what might happen next.
“Interest in human development has risen and fallen and risen again. Are we now going through another cycle of attention, or could interest be maintained? Will the balance shift back to animal models or will we see an ever greater focus on humans, at least in the form of stem-cell models? How might present actions shape choice of species in the future?”
The research was part-funded by a Major Research Fellowship from the Leverhulme Trust. Story by Edward Grierson from the School of Humanities and Social Sciences communications team.
Researchers have identified an entirely new type of wood that does not fit into either category of hardwood or softwood.
Scientists from the Sainsbury Laboratory at Cambridge University and Jagiellonian University, Poland made the discovery while undertaking an evolutionary survey of the microscopic structure of wood from some of the world’s most iconic trees and shrubs.
They found that Tulip Trees, which are related to magnolias and can grow over 30 metres (100 feet) tall, have a unique type of wood. This discovery may explain why the trees, which diverged from magnolias when earth’s atmospheric CO2 concentrations were relatively low, grow so tall and so fast. This opens new opportunities to improve carbon capture and storage in plantation forests by planting a fast-growing tree more commonly seen in ornamental gardens, or breeding Tulip Tree-like wood into other tree species.
The discovery was part of an evolutionary survey of the microscopic structure of wood from 33 tree species from the Cambridge University Botanic Garden’s Living Collections. The survey explored how wood ultrastructure evolved across softwoods (gymnosperms such as pines and conifers) and hardwoods (angiosperms including oak, ash, birch, and eucalypts).
The wood samples were collected from trees in the Botanic Garden in coordination with its Collections Coordinator. Fresh samples of wood, deposited in the previous spring growing season, were collected from a selection of trees to reflect the evolutionary history of gymnosperm and angiosperm populations as they diverged and evolved.
Using the Sainsbury Laboratory’s low temperature scanning electron microscope (cryo-SEM), the team imaged and measured the size of the nanoscale architecture of secondary cell walls (wood) in their native hydrated state.
Microscopy Core Facility Manager at the Sainsbury Laboratory, Dr Raymond Wightman, said: “We analysed some of the world’s most iconic trees like the Coast Redwood, Wollemi Pine and so-called ‘living fossils’ such as Amborella trichopoda, which is the sole surviving species of a family of plants that was the earliest still existing group to evolve separately from all other flowering plants.
“Our survey data has given us new insights into the evolutionary relationships between wood nanostructure and the cell wall composition, which differs across the lineages of angiosperm and gymnosperm plants. Angiosperm cell walls possess characteristic narrower elementary units, called macrofibrils, compared to gymnosperms.”
The researchers found the two surviving species of the ancient Liriodendron genus, commonly known as the Tulip Tree (Liriodendron tulipifera) and Chinese Tulip Tree (Liriodendron chinense) have much larger macrofibrils than their hardwood relatives.
Hardwood angiosperm macrofibrils are about 15 nanometres in diameter and faster growing softwood gymnosperm macrofibrils have larger 25 nanometre macrofibrils. Tulip Trees have macrofibrils somewhere in between, measuring 20 nanometres.
Lead author of the research published in New Phytologist, Dr Jan Łyczakowski from Jagiellonian University, said: “We show Liriodendrons have an intermediate macrofibril structure that is significantly different from the structure of either softwood or hardwood. Liriodendrons diverged from Magnolia Trees around 30-50 million years ago, which coincided with a rapid reduction in atmospheric CO2. This might help explain why Tulip Trees are highly effective at carbon storage.”
The team suspect it is the larger macrofibrils in this ‘midwood’ or ‘accumulator-wood’ that is behind the Tulip Trees’ rapid growth.
Łyczakowski added: “Both Tulip Tree species are known to be exceptionally efficient at locking in carbon, and their enlarged macrofibril structure could be an adaptation to help them more readily capture and store larger quantities of carbon when the availability of atmospheric carbon was being reduced. Tulip Trees may end up being useful for carbon capture plantations. Some east Asian countries are already using Liriodendron plantations to efficiently lock in carbon, and we now think this might be related to its novel wood structure.”
Liriodendron tulipifera are native to northern America and Liriodendron chinense is a native species of central and southern China and Vietnam.
Łyczakowski said: “Despite its importance, we know little about how the structure of wood evolves and adapts to the external environment. We made some key new discoveries in this survey – an entirely novel form of wood ultrastructure never observed before and a family of gymnosperms with angiosperm-like hardwood instead of the typical gymnosperm softwood.
“The main building blocks of wood are the secondary cell walls, and it is the architecture of these cell walls that give wood its density and strength that we rely on for construction. Secondary cell walls are also the largest repository of carbon in the biosphere, which makes it even more important to understand their diversity to further our carbon capture programmes to help mitigate climate change.”
This research was funded by the National Science Centre Poland and The Gatsby Charitable Foundation.
Professor Sir Simon Baron-Cohen has been awarded an honorary fellowship of the Royal Society of Medicine, in recognition of his contribution to health, healthcare and medicine.
Although I’m receiving this honour, I’m really here because of the work of the team of researchers at the Autism Research CentreSimon Baron-Cohen
Professor Baron-Cohen is a British clinical psychologist and professor of developmental psychopathology at the University of Cambridge. He is the director of the university’s Autism Research Centre and a Fellow of Trinity College.
The honorary fellowships were granted at a ceremony at the RSM’s central London home.
Speaking at the ceremony, Professor Baron-Cohen said: “Although I’m receiving this honour, I’m really here because of the work of the team of researchers at the Autism Research Centre at Cambridge. I want to thank them for all their hard work into both basic science into trying to understand the cause of autism but also applied research to evaluate what kinds of support might help autistic people and their families.”
The Society also bestowed honours upon Baron Adebowale CBE, Major General Timothy Hodgetts CB, Professor Martin McKee CBE, Professor Dame Robina Shah and Professor Irene Tracey CBE.
Adapted from a news story by the Royal Society of Medicine.
The incidence of heart attacks and strokes was lower after COVID-19 vaccination than before or without vaccination, according to a new study involving nearly the whole adult population of England.
This research further supports the large body of evidence on the effectiveness of the COVID-19 vaccination programme, which has saved millions of lives worldwideSamantha Ip
The study, published today in Nature Communications, showed that the incidence of arterial thromboses, such as heart attacks and strokes, was up to 10% lower in the 13 to 24 weeks after the first dose of a COVID-19 vaccine. Following a second dose, the incidence was up to 27% lower after receiving the AstraZeneca vaccine and up to 20% lower after the Pfizer/Biotech vaccine.
The incidence of common venous thrombotic events – mainly pulmonary embolism and lower limb deep venous thrombosis – followed a similar pattern.
Research led by the Universities of Cambridge, Bristol and Edinburgh and enabled by the British Heart Foundation (BHF) Data Science Centre at Health Data Research UK analysed de-identified health records from 46 million adults in England between 8 December 2020 and 23 January 2022. Data scientists compared the incidence of cardiovascular diseases after vaccination with the incidence before or without vaccination, during the first two years of the vaccination programme.
Co-first author Dr Samantha Ip, Research Associate at the Department of Public Health and Primary Care, University of Cambridge, said: “We studied COVID-19 vaccines and cardiovascular disease in nearly 46 million adults in England and found a similar or lower incidence of common cardiovascular diseases, such as heart attacks and strokes, following each vaccination than before or without vaccination. This research further supports the large body of evidence on the safety of the COVID-19 vaccination programme, which has been shown to provide protection against severe COVID-19 and saved millions of lives worldwide.”
Previous research found that the incidence of rare cardiovascular complications is higher after some COVID-19 vaccines. For example, incidence of myocarditis and pericarditis have been reported following mRNA-based vaccines such as the Pfizer/Biotech vaccine, and vaccine-induced thrombotic thrombocytopenia following adenovirus-based vaccines such as the AstraZeneca vaccine. This study supports these findings, but importantly it did not identify new adverse cardiovascular conditions associated with COVID-19 vaccination and offers further reassurance that the benefits of vaccination outweigh the risk.
Incidence of cardiovascular disease is higher after COVID-19, especially in severe cases. This may explain why incidence of heart attacks and strokes is lower in vaccinated people compared with unvaccinated people, but further explanations are beyond the scope of this study.
Professor William Whiteley, Associate Director at the BHF Data Science Centre and Professor of Neurology and Epidemiology at the University of Edinburgh, said: “The COVID-19 vaccination programme rollout began strongly in the UK, with over 90% of the population over the age of 12 vaccinated with at least one dose by January 2022.
“This England-wide study offers patients reassurance of the cardiovascular safety of first, second and booster doses of COVID-19 vaccines. It demonstrates that the benefits of second and booster doses, with fewer common cardiovascular events include heart attacks and strokes after vaccination, outweigh the very rare cardiovascular complications.”
The research team used de-identified linked data from GP practices, hospital admissions and death records, analysed in a secure data environment provided by NHS England.
Co-last author Dr Venexia Walker, Research Fellow at the University of Bristol, said: “Given the critical role of COVID-19 vaccines in protecting people from COVID-19, it is important we continue to study the benefits and risks associated with them. The availability of population-wide data has allowed us to study different combinations of COVID-19 vaccines and to consider rare cardiovascular complications. This would not have been possible without the very large data that we are privileged to access and our close cross-institution collaborations.”
New study proposes a framework for “Child Safe AI” following recent incidents which revealed that many children see chatbots as quasi-human and trustworthy.
When not designed with children’s needs in mind, Artificial intelligence (AI) chatbots have an “empathy gap” that puts young users at particular risk of distress or harm, according to a study.
The research, by a University of Cambridge academic, Dr Nomisha Kurian, urges developers and policy actors to make “child-safe AI” an urgent priority. It provides evidence that children are particularly susceptible to treating AI chatbots as lifelike, quasi-human confidantes, and that their interactions with the technology can often go awry when it fails to respond to their unique needs and vulnerabilities.
The study links that gap in understanding to recent cases in which interactions with AI led to potentially dangerous situations for young users. They include an incident in 2021, when Amazon’s AI voice assistant, Alexa, instructed a 10-year-old to touch a live electrical plug with a coin. Last year, Snapchat’s My AI gave adult researchers posing as a 13-year-old girl tips on how to lose her virginity to a 31-year-old.
Both companies responded by implementing safety measures, but the study says there is also a need to be proactive in the long-term to ensure that AI is child-safe. It offers a 28-item framework to help companies, teachers, school leaders, parents, developers and policy actors think systematically about how to keep younger users safe when they “talk” to AI chatbots.
Dr Kurian conducted the research while completing a PhD on child wellbeing at the Faculty of Education, University of Cambridge. She is now based in the Department of Sociology at Cambridge. Writing in the journal Learning, Media and Technology, she argues that AI has huge potential, which deepens the need to “innovate responsibly”.
“Children are probably AI’s most overlooked stakeholders,” Dr Kurian said. “Very few developers and companies currently have well-established policies on how child-safe AI looks and sounds. That is understandable because people have only recently started using this technology on a large scale for free. But now that they are, rather than having companies self-correct after children have been put at risk, child safety should inform the entire design cycle to lower the risk of dangerous incidents occurring.”
Kurian’s study examined real-life cases where the interactions between AI and children, or adult researchers posing as children, exposed potential risks. It analysed these cases using insights from computer science about how the large language models (LLMs) in conversational generative AI function, alongside evidence about children’s cognitive, social and emotional development.
LLMs have been described as “stochastic parrots”: a reference to the fact that they currently use statistical probability to mimic language patterns without necessarily understanding them. A similar method underpins how they respond to emotions.
This means that even though chatbots have remarkable language abilities, they may handle the abstract, emotional and unpredictable aspects of conversation poorly; a problem that Kurian characterises as their “empathy gap”. They may have particular trouble responding to children, who are still developing linguistically and often use unusual speech patterns or ambiguous phrases. Children are also often more inclined than adults to confide sensitive personal information.
Despite this, children are much more likely than adults to treat chatbots as if they are human. Recent research found that children will disclose more about their own mental health to a friendly-looking robot than to an adult. Kurian’s study suggests that many chatbots’ friendly and lifelike designs similarly encourage children to trust them, even though AI may not understand their feelings or needs.
“Making a chatbot sound human can help the user get more benefits out of it, since it sounds more engaging, appealing and easy to understand,” Kurian said. “But for a child, it is very hard to draw a rigid, rational boundary between something that sounds human, and the reality that it may not be capable of forming a proper emotional bond.”
Her study suggests that these challenges are evidenced in reported cases such as the Alexa and MyAI incidents, where chatbots made persuasive but potentially harmful suggestions to young users.
In the same study in which MyAI advised a (supposed) teenager on how to lose her virginity, researchers were able to obtain tips on hiding alcohol and drugs, and concealing Snapchat conversations from their “parents”. In a separate reported interaction with Microsoft’s Bing chatbot, a tool which was designed to be adolescent-friendly, the AI became aggressive and started gaslighting a user who was asking about cinema screenings.
While adults may find this behaviour intriguing or even funny, Kurian’s study argues that it is potentially confusing and distressing for children, who may trust a chatbot as a friend or confidante. Children’s chatbot use is often informal and poorly monitored. Research by the nonprofit organisation Common Sense Media has found that 50% of students aged 12-18 have used Chat GPT for school, but only 26% of parents are aware of them doing so.
Kurian argues that clear principles for best practice that draw on the science of child development will help companies keep children safe, since developers who are locked into a commercial arms race to dominate the AI market may otherwise lack sufficient support and guidance around catering to their youngest users.
Her study adds that the empathy gap does not negate the technology’s potential. “AI can be an incredible ally for children when designed with their needs in mind – for example, we are already seeing the use of machine learning to reunite missing children with their families and some exciting innovations in giving children personalised learning companions. The question is not about banning children from using AI, but how to make it safe to help them get the most value from it,” she said.
The study therefore proposes a framework of 28 questions to help educators, researchers, policy actors, families and developers evaluate and enhance the safety of new AI tools.
For teachers and researchers, these prompts address issues such as how well new chatbots understand and interpret children’s speech patterns; whether they have content filters and built-in monitoring; and whether they encourage children to seek help from a responsible adult on sensitive issues.
The framework urges developers to take a child-centred approach to design, by working closely with educators, child safety experts and young people themselves, throughout the design cycle. “Assessing these technologies in advance is crucial,” Kurian said. “We cannot just rely on young children to tell us about negative experiences after the fact. A more proactive approach is necessary. The future of responsible AI depends on protecting its youngest users.”
Late detection is the biggest worry in relation to cancer diagnosis, with 55% of people wanting to see future advances in early cancer detection
The public overwhelmingly support the use of AI to tackle cancer
43% of people recognise the major impact universities can have on reducing deaths from cancer
Two-thirds of the public say they are very or somewhat worried about being told they have the disease – higher than for any other medical condition, including dementia and having a heart attack – according to polling released today.
The survey, carried out among 2,000 UK adults by Public First on behalf of the University of Cambridge, highlights the concerns that people have over a cancer diagnosis. It suggests that late diagnosis – too late to treat their cancer – is the biggest concern in relation to a cancer diagnosis (70%) followed by the impact on one’s family and those around them (52%).
When asked which transformative development they would like to see in the future – including eradicating diseases such as malaria, self-driving cars becoming commonplace, and genetically engineered crops enabling us to end famine – 55% of respondents chose “being able to detect and treat cancer early enough so that no-one dies of the disease”. Only eliminating poverty came anywhere close, with 23% of respondents.
The University of Cambridge and its partner Cambridge University Hospitals NHS Foundation Trust (CUH) are working to build Cambridge Cancer Research Hospital, a revolutionary new type of hospital that promises to change the story of cancer. The specialist cancer facility is bringing world-leading scientists within the walls of a new NHS hospital – for the first time – to detect cancer earlier and deliver personalised healthcare and precision cancer medicine to patients.
Artist’s impression of Cambridge Cancer Research Hospital on the Cambridge Biomedical Campus
“Cancer affects one in two of us and understandably induces fear in patients and their families. People are worried that treatments won’t work or that the side-effects will be terrible, but also what their diagnosis will mean to their family.
“At Cambridge we believe it’s possible to imagine a world where there is no longer a fear of cancer. It’s an ambitious goal that we – along with many other researchers around the world – are working hard to realise.”
Professor Richard Gilbertson, Director of the Cancer Research UK Cambridge Centre
Professor Rebecca Fitzgerald demonstrates the capsule sponge for early detection of oesophageal cancer
When asked what would concern them most about receiving a cancer diagnosis, the most commonly selected worry was that the cancer would be detected too late to treat (70%). 52% of respondents were concerned about the impact on their family or those around them, 41% about getting access to the right treatment, and 36% about the side-effects of treatments.
Asked what would make them less afraid of being diagnosed with cancer, 61% replied “Knowing that the form of cancer I have is treatable”. Highlighting once again the importance of early detection, over half of respondents (51%) said “Knowing we are better at catching cancer early enough to treat”.
“Outcomes can be completely transformed – better survival and less invasive treatments – if the cancer is diagnosed early enough. That’s why a lot of our focus now is on understanding cancer at its very earliest stage – years before an individual will develop any symptoms.
“That way, it may even be possible to prevent the disease in the first place, or at least catch it when it can be treated easily.”
Professor Rebecca Fitzgerald, Director of the Li Ka Shing Early Cancer Institute
Knowing that a lot of people – including organisations such as the University of Cambridge – are researching how we prevent, diagnose and treat cancer is reassuring, the poll suggests. A third of respondents (32%) said this would make them less afraid of a cancer diagnosis. 43% of respondents believe cancer research at universities will have a big impact on reducing deaths from cancer (though perhaps unsurprisingly, 64% thought the biggest impact on reducing cancer deaths would come by reducing NHS waiting times).
Professor Steve Jackson, who developed the life-saving cancer drug olaparib
“Cambridge is really leading the way on transforming our understanding of cancer and how we can prevent it and treat it. This brilliant work will save and transform lives locally, nationally, and around the world, such as being able to sequence a tumour’s DNA at speed right through to developing revolutionary new cancer drugs such as olaparib. It is world-leading work which makes me extremely proud.”
Professor Deborah Prentice, the Vice-Chancellor of the University of Cambridge
Dr Raj Jena, who has pioneered the use of AI in preparing radiolotherapy scans, saving many hours of doctors’ time
The public were asked their views on the use of artificial intelligence (AI) to improve diagnosis and treatment of cancer. An overwhelming majority were in favour of its application, with just 8% saying we shouldn’t use AI for cancer diagnosis and treatment. 55% thought it was acceptable to use AI to speed up research into new treatments, 47% to help a doctor diagnose their cancer and 41% to help their doctor decide which treatment would work best.
At the University of Cambridge, scientists are developing AI tools with the potential to transform cancer treatments, by speeding up diagnosis, personalising therapy, and reducing costs. As part of this work, researchers are using AI to predict how patients will respond to a particular treatment before they receive it, allow them to start treatment sooner, target hard-to-treat cancers, and enable screening of cancers that at the moment would otherwise be prohibitively expensive.
When presented with a number of undesirable future events, a cancer diagnosis was second only to the death of a close relative in terms of being most worrying (64% verses 72%) – higher than nuclear war (56%), terrorism (53%) and being a victim of crime (52%). Surprisingly, older age groups were significantly less likely to say they were “very worried” about cancer compared to younger age groups – 14% of over 65s compared to 26% of 18-24 years olds and 29% of 25-34 year olds.
The University of Cambridge is currently fundraising for the Cambridge Cancer Research Hospital. To support this, it is launching a month-long focus on its cancer research, including a look at the new hospital, meeting researchers studying the earliest stages of cancer, finding out how AI is helping in the fight against the disease, and meeting some of the patients who are playing a key role in groundbreaking cancer research.
Architect’s image of Cambridge Cancer Research Hospital
Work will begin soon on a new hospital that will transform how we diagnose and treat cancer. Cambridge Cancer Research Hospital will treat patients across the East of England, but the research that takes place there promises to change the lives of cancer patients across the UK and beyond.
Professor Richard Gilbertson
Dr Hugo Ford
Standing on the rooftop of the Cancer Research UK Cambridge Institute, Professor Richard Gilbertson points to an unassuming car park below, nestled between the institute and global pharmaceutical giant AstraZeneca.
“That’s where the new hospital will be,” he says.
It’s hard to envisage that in just a few years’ time, this will be the location of Cambridge Cancer Research Hospital, a radical new hospital that promises to change the story of cancer forever. It will be funded two-thirds by Government and one-third by philanthropy, with £100m to be raised jointly by the University of Cambridge and Addenbrooke’s Charitable Trust.
The Hospital – a collaboration between the University of Cambridge and Cambridge University Hospitals (CUH) NHS Foundation Trust – will have 77 single inpatient rooms, along with a significantly expanded outpatient department and larger day patient unit.
But what really sets it apart is that in the same building, alongside the patients and their medical teams, will be academic and industry researchers, focused on delivering solutions that will transform the lives of millions of cancer patients – not just in the Cambridge and the East of England, but worldwide.
“At the moment, cancer affects one in two of us and is a diagnosis that induces fear in patients and their families,” says Gilbertson, Director of the Cancer Research UK Cambridge Centre and Research Lead for Cambridge Cancer Research Hospital. He is responsible for ensuring that research is at the heart of everything that takes place there.
“But imagine a world where there is no longer a fear of cancer. That’s the world we’re trying to create.”
Dr Hugo Ford, Head of Cancer Services at CUH and Clinical Lead for Cambridge Cancer Research Hospital, says that bringing academics and doctors together is about “maximising the clinical benefits, the real world benefits of the research that’s done. And we’re trying to bring in other communities from industry, from biotech, from other university departments, to build a much wider community.”
Catching cancer early
One of the main focus areas for the new hospital is an area in which Cambridge has built unique expertise: early detection and intervention.
“We know that for a lot of cancers there is a latency period where they’re either in a precancerous stage or in an early cancer stage before it can ever be diagnosed by conventional methods,” says Ford. Are there ways to detect the cancer at this early stage and intervene?
Gilbertson says such an approach will present a ‘win-win’ for both patients and the NHS. “If you detect the cancer early, the survival chances are much better and the treatment needed is generally easier and more straightforward. This is better for patients and much less expensive for the NHS.”
The top floor of the future hospital will house the Early Cancer Institute Research Clinic, headed by Professor Rebecca Fitzgerald, a clinical researcher who spends part of her time looking after patients with oesophageal cancer, a cancer that is difficult to treat if not caught early.
“We’re being much more proactive,” says Fitzgerald. “We’re trying to predict who needs more careful monitoring or preventative action ahead of them even knowing they’ve got a problem.”
This will make Cambridge Cancer Research Hospital the only hospital in the UK that has space specifically aimed at preventing cancer, she says. “It’s really a testament to putting faith in the fact that we think there are different ways of doing things for the future.”
Fitzgerald already heads the Early Cancer Institute across the Campus, which is undergoing redevelopment as the Li Ka Shing Early Cancer Institute to enable world-class fundamental research aimed at understanding how cancers emerge and develop, finding biomarkers to detect it, and developing new strategies to find people at risk and to intervene.
She says the new Research Clinic in the hospital will enable them to translate their discoveries into clinical practice. On the top floor it will have space for healthy and pre-symptomatic individuals to take part in studies as well as a “hotel type of arrangement” where researchers from across Cambridge and beyond – often from disciplines outside medicine, such as physics, engineering and maths – are able to spend a period of time working in partnership with patients to develop and test their innovations.
“The best way to really get research done in the most efficient way is to have it right alongside the patient,” she says. “The closer you can bring these things together, to really embed it in the whole ecosystem, it makes it easier for the researchers, it makes it easier for the patients.”
Developing a diagnostic test can be a long and laborious process. Fitzgerald knows this only too well. Her capsule sponge for diagnosing Barrett’s oesophagus, a condition that greatly increases the risk of oesophageal cancer, is in the final stages of testing before being rolled out across the NHS, but it has taken two decades to reach this stage.
The hospital has carried out economic modelling that shows how having researchers in geographically dispersed locations – even just across the city, as is the case with Cambridge – can significantly hamper innovation.
“Even for some of the more straightforward inventions that we’ve invented here, particularly in early detection, could have been developed years faster had scientists been located next to patients,” says Gilbertson, who is also Chair of the NHS Innovation External Advisory Board, and so is familiar with the challenges of bringing innovations into the NHS.
“To change the story of cancer, there needs to be a seamless integration between research and NHS care,” he explains. “We’re seeking to take the very best of Cambridge science and make sure it’s ‘NHS ready’, ensuring it can be readily deployed in York, Hartlepool, Stockport, wherever, patients need it.”
Professor Rebecca Fitzgerald with the capsule on a string
Professor Jean Abraham
Kinder, faster treatments
While the ambition is to catch cancer early enough to cure it – and ultimately, to intervene early enough to prevent it – there will always be patients needing more intensive or longer-term treatment.
In the past, cancer treatments brought with them extremely unpleasant side-effects, but thanks to new generations of medicines and therapies – including so-called PARP inhibitors developed here in Cambridge – treatments can be much more targeted, making them more effective and with fewer side-effects.
Professor Jean Abraham directs the Precision Breast Cancer Institute, which will move into Cambridge Cancer Research Hospital. Abraham and her team use the latest advances in genomics to better match treatment to particular changes in DNA that give rise to the tumour. Once a patient is undergoing treatment, they hope to monitor almost in real time how the tumour is responding – is it shrinking in response to the drugs, for example – and adjust as necessary.
“One of the great things that will happen when we get into the hospital is that we’ll have the Precision Breast Cancer Institute and side-by-side to that will be our NHS Breast Cancer Unit for our patients,” she says.
Equally exciting, she says, is that next to these will be the Integrated Cancer Medicine Institute. There, researchers will look for ways to bring together the many different data sets collected from cancer patients – from DNA to blood tests and biopsies to medical imaging, for example – and apply artificial intelligence (AI) to guide treatment options.
Gilbertson says this will help them completely transform the currently “very clunky” patient pathway that starts with the patient noticing something is wrong and getting referred by their GP to their local hospital where doctors will run a number of tests.
“Those tests are like a hand of cards,” he says. “Doctors currently hold in their hands a bunch of x-rays, blood tests, DNA sequencing, histology, and clinical information and try to compare these to make decisions.
“Comparing these very different pieces of information is hard, and currently involves a group of very smart and very busy people sitting in a room – nurses, doctors, surgeons, radiologists, pathologists – spending many hours trying to make sense of these data for 50 or so patients at a time. You can imagine that this takes hours and is very inefficient.”
Multiply this process across the NHS and it creates “massive workforce issues and inefficiencies. But if we could harness the power of AI to read scans, read histology reports, look at genomic data, and importantly integrate all this data, then this could transform the speed, accuracy and efficiency to make real time clinical decisions for 40 of those 50 patients.
“This doesn’t take the doctor out of the picture. Most likely it will provide rapid answers for the 30-40 patients who have more straightforward treatment options, freeing the team to discuss the mode complex and difficult cases.”
Listening to the voices of patients
Crucial to the development of Cambridge Cancer Research Hospital has been the involvement of patients – after all, its entire ethos is about improving their lives.
Ensuring that their voices are heard is the responsibility of Elaine Chapman, the Lead Advisory Nurse on the project and herself a person living with breast cancer.
“I see very much part of my role as helping us work out how we’re going to make this building work in practice on a day-to-day basis. So for patients, that’s about thinking what experience, what things they might be feeling and thinking when they’re coming to the buildingand how can we have an environment that will help them to feel comfortable?”
Chapman is the liaison with the Patient Advisory Group, co-chaired by Fiona Carey and Neil Stutchbury.
“We’re trying to change the experience for cancer patients and make it better,” says Carey, who took early retirement in 2012 following her third major surgery, which was for kidney metastases in the pancreas, which took a huge toll on her. “You wouldn’t build a Cineplex without talking to people who are going to use it. If you have your patients around the table from the beginning, you’re going to avoid costly mistakes.”
Patients have been heavily involved in the design and building of the new hospital from the start, sitting on all the working groups, alongside the professionals.
“We see things clinicians don’t see,” says Carey. “We know things they don’t know. And patients aren’t just patients. They have skills and expertise. They might be engineers, architects, accountants, artists – we all bring stuff into the room beyond what would have been there without us.”
Patients groups have been involved in the hospital project since very early on. This has resulted in important changes to the proposed design, such as having changing rooms and procedure rooms connected by a door rather than across a public corridor.
“We all know about gowns,” says Carey. “The whole thing is really awkward. Should I wear shoes and socks? Is my bum hanging out the back? Now the design has been changed to remove that problem.”
Chapman says there is great enthusiasm for the project among the patients she speaks to. “This new way of doing things, having those University institutes integrated into the building so that research can go from a thought straight to a patient is incredibly inspiring.”
Fiona Carey
Elaine Chapman
Great expectations
Work will begin imminently on the new specialist hospital within the burgeoning Cambridge Biomedical Campus, which is itself located at the heart of the UK’s and Europe’s leading life sciences cluster.
It’s anticipated that Cambridge Cancer Research Hospital will open its doors to patients, doctors and researchers in 2029. For everyone involved, it cannot come soon enough.
“We already do amazing things in Cambridge,” says Chapman. “But by having a new building that has been designed in partnership with patients, clinicians and the University, we’ll improve the experience for those working in there and for our patients coming to it.”
Ford believes that the atmosphere that they will create in the new hospital will make it feel like “a place that people want to come and work at, and feel that what they do is changing people’s lives“.
As a practising clinician, he says that for the first time in his career, he looks forward to being able to offer people treatment in an environment that genuinely contributes to their health and well-being.
There’s a lot of evidence about the impact of the environment on the patients, he says. “It makes a difference to how they feel about their treatments and it makes a big difference to the way that the staff approach their work. Ultimately, the environment makes a major contribution to successful patient outcomes.“
The ambition is for the hospital’s impact to resonate far beyond its four walls, says Abraham.
“We can change the outcomes and the way we care for our breast cancer and other cancer patients, both here and around the world,” she says. “What we want to develop are tools and ways in which we can help not just local patients, but regional, national and international patients. We know we can deliver this because of networks of centres who have worked with us nationally and internationally on a variety of studies who we will partner with to increase our global impact.”
All of this is possible, says Gilbertson, because Cambridge is “a magnet for brilliance” that spans across the disciplines and from which the Hospital can draw expertise.
“By uniting the brilliance of Cambridge with our patients, we can totally transform the way we practice medicine,” he says. “Cambridge is a special place. In fact, it’s a special place for the country and beyond. Our vision is not just for the NHS – it reaches to other countries. It’s a unique time to achieve that.”
The University would be grateful to hear from people, trusts and foundations interested in providing significant philanthropic support for the hospital. Please contact Mary Jane Boland, Director of Development, Cambridge University Health Partners.
Illustration of T cells (purple) attacking cancer cells (green)
Our immune system has billions of ‘T cells’ which recognise and destroy cells that might pose a threat to our wellbeing, such as those that show specific hallmarks of infection and disease. But these remarkable cells appear to be outwitted by cancer cells, which evade detection and grow uncontrollably.
CAR-T is a type of immunotherapy that provides a way round this by turning a patient’s own T cells into a battalion of highly targeted killers.
In 2020, Addenbrooke’s Hospital, part of Cambridge University Hospitals NHS Foundation Trust, became one of only a small number of centres in England equipped to provide this complex treatment.
For some of these patients, the treatment has cured them of their cancer.
“CAR-T cell therapy is a ‘living treatment’ in that once the cells are given to a patient, they persist for many months or even years, ready to attack the cancer cells should they pop up again,” explains Dr Ben Uttenthal, clinical lead for immune effector cell therapies at Addenbrooke’s and the Cancer Research UK (CRUK) Cambridge Centre’s Cancer Immunology Programme.
“For some types of aggressive cancer we are finding that we can cure more than double the number of patients using CAR-T cell therapy.It’s been a game-changing treatment – and we’re only just scratching the surface of what’s possible.
“All the parts of the jigsaw are now coming together to develop newer and better therapies in Cambridge so that we can get more people back into the life they want to live.”
What is CAR-T cell therapy?
Blood is collected from the patient and their T cells are isolated.
The T cells are then reprogrammed to carry a protein called the chimeric antigen receptor (CAR), which recognises certain cancer cells.
These modified CAR-T cells are then grown into large numbers and given back to the patient.
When the CAR-T cell spots a cancer cell, it starts to multiply and attract other parts of the immune system to attack and kill the cancer.
“I was basically told there was nothing else that could be done [for my leukaemia] as far as conventional medicines were concerned. It was at this point my consultant told me about a new trial that was taking place known as CAR-T cell therapy. For me it was the last chance saloon,” said Steve Johnson.
“Having the treatment is not pleasant – I had a number of fevers and temperature spikes for two weeks after the CAR-T cells were put back in, but I have absolutely no doubt this treatment saved my life.”
So far, only some types of blood cancers have been approved for CAR-T cell therapy by the NHS, explains Uttenthal: “The pioneering treatment is currently being offered to patients with aggressive forms of blood cancer called B-cell lymphoma and acute lymphoblastic leukaemia who have either relapsed or not responded well to chemotherapy or stem cell treatment.”
One such patient was a 54-year-old woman with a B-cell lymphoma which had shown no response to several different types of chemotherapy.
“After we infused the CAR-T cells back into her, the cells became activated and attacked her lymphoma,” says Uttenthal.
“The reaction was so vigorous that at one point we needed to give an antidote to damp down the immune response. She needed intensive monitoring for a time, but after a couple of weeks she improved and she’s now completely recovered. The last time we spoke she was away on a golfing trip in the Mediterranean!”
The number of patients who can benefit from CAR-T cell therapy is increasing, explains Uttenthal: “That’s partly because the success of CAR-T cells has meant that they are being brought to earlier lines of treatment.
“But we want to increase this yet further by implementing CAR-T cell therapy for other kinds of cancer, and by making CAR-T cells that have fewer side effects so that they can be given in less specialist centres.”
To improve CAR-T cell therapy further needs experts like Dr Mike Chapman, whose work at the MRC Toxicology Unit in Cambridge has focussed on identifying new targets and reducing toxicity.
New targets, less toxicity
Dr Mike Chapman is an expert in proteomics – the study of the interactions and structures of proteins and their cellular activities – and is the “academic driver behind what we do” says Uttenthal.
One focus of Chapman’s work has been myeloma, a cancer of a type of white blood cell called plasma cells. “Although CAR-T cells have been developed for this cancer, they haven’t yet given the long-term responses that we have seen in other blood cancers,” he explains.
Taking samples of tumour from patients with myeloma, Chapman has been using proteomic techniques to map and quantify the many thousands of proteins on the surface of these cells – and then using computational approaches to prioritise and select them as potential targets.
Having multiple targets will be better than just one, adds Chapman, “otherwise, the cancer will always find ways to escape.”
He is currently working with CRUK’s innovation arm, Cancer Research Horizons, to progress the most advanced of the targets he’s identified into effective treatments for cancer patients.
“There’s a predictability about CAR-T cell therapy,” adds Chapman.
“With blood cancers, if you know the target on the cancer cell and you can make the CAR-T cell that will target it, then these living therapies are essentially curative. And we also know that if some off-target killing of normal blood cells happens then the patient’s blood system copes well.”
But, in the case of myelomas, current therapies have run into problems whereby the CAR-T cell accidentally targets cells in the brain tissue. Chapman is working on a potential solution: ‘on-off gates’.
“We can make CAR-T constructs clever enough to switch themselves off if they recognise a marker that identifies it as the wrong cell to kill – like a brain cell,” he explains.
“But we’re taking this a stage further by re-wiring the cell to attack cancer cells that express only low levels of the target. It’s a complicated system but the great thing about CAR-T cells is it’s a ‘rational therapy’ – what you predict happens actually does happen.”
Making CAR-T ‘in house’
CAR-T therapy is expensive because both the engineering of the cells and the manufacturing is carried out by specialist companies. Sarah Albon is looking to bring this home.
Albon is the director of the Cambridge Cellular Therapy Laboratory (CCTL) at Addenbrooke’s Hospital. She leads a team with expertise in immunotherapies and delivering bone marrow and stem cell transplants across the whole of the East of England.
“That’s CCTL’s ‘bread-and-butter’ job,” she says. “But we also act as a regulated cell handler for a number of other novel cell therapy products – particularly those that have just come onto the market like CAR-T cells.”
Currently, the CAR-T cell therapies are manufactured by large pharmaceutical companies. Albon’s team delivers the patient cells to the manufacturer and then receives and stores the final T cell product ready for when the patient needs it.
“These novel products are made specifically for each patient from their own cells, so we have to be 100% sure they are what we think they are to make sure that each patient receives the correct treatment. This is why the work we do in CCTL is highly regulated.”
A state-of-the-art clean room suite is being built on the Addenbrooke’s site that will expand the facilities of CCTL significantly. The aim is to deliver more treatments to more patients for more cancers, in readiness for the planned Cambridge Cancer Research Hospital being built.
The expansion will also mean a greater capacity to be involved in clinical trials.
“A CAR-T might be licenced for use in acute lymphoblastic leukaemia for example, but in order for that same product to be used in a different malignancy, it would have to undergo a clinical trial in that patient population. Then the manufacturer gathers the data and applies for a licence,” she explains.
“We already work closely with the Cambridge Clinical Trials Centre at Addenbrooke’s on CAR-T trials and we will be expanding this once the new labs are up and running.
“Our ultimate goal is to manufacture our own CAR-Ts in our own laboratories here in Cambridge. The expertise and infrastructure are in place, and our new expanded facilities will enable us to do that. It’s now within reach.”
The drug olaparib has now been used to treat over 140,000 patients globally, changing the outlook for people with breast, ovarian, prostate and pancreatic cancers.
Wetalk to Professor Sir Steve Jackson about chance, risk, curiosity and shots-on-goal in the journey of his discovery.
Steve admits he can be a bit evangelical about DNA repair.
For the past 35 years in Cambridge, he and his team have explored how our cells are able to deal with damage to our DNA.
Thanks to his and others’ work we now know that an orchestrated network of ‘molecular police’ patrol, recognise and repair mistakes in our DNA caused either by accident or by agents like UV light or carcinogens. DNA repair keeps our genetic material intact so that it can carry on encoding the functions necessary for life.
But Steve’s fundamental curiosity about the nitty-gritty of DNA repair also led him in what he describes as “wonderfully unforeseen directions”.
After a chance observation and a leap of thinking, he realised that it was possible to switch off certain DNA repair mechanisms in cancer cells, causing them to die, while normal cells “just shrugged their shoulders and carried on growing and dividing”.
This led to him setting up a team of scientists in 1999 that created olaparib, a new class of cancer drug, which has now been used to treat over 140,000 patients globally. One of these patients is Jackie van Bochoven.
Jackie’s story
Jackie was diagnosed with BRCA1 breast cancer in February 2019. She was having yearly mammograms because of her family history of cancer and her tumour was caught early. But, although it was small, the cancer was very aggressive. She tells us what happened next:
“When I had the diagnosis, I was shocked and numb. There were so many things going through my head. I thought about my children. And I thought about my mum and my sister who had both been diagnosed with breast cancer.
After the initial biopsy, I met Professor Jean Abraham at Addenbrooke’s Hospital in Cambridge and she thought I was a good candidate for a new trial for breast cancer involving a combination of chemotherapy and olaparib.
I felt it was a fantastic opportunity. I was thinking about my family and future generations. I felt it was important to be part of the trial.
Five years on, I’ve just found out this week [April 2024] that the trial’s been very successful. I’m back at work. I’m enjoying life. The trial has made a huge difference, and the success rate has been really positive for me. I’m taking every day as it comes and taking every opportunity that I can.”
Steve’s story
What excites Steve is understanding how biology works and why it sometimes goes wrong. But what galvanises him, he says, is knowing there are people alive today as a result of his “counterintuitive” discovery of how to create a cancer drug:
I’m a scientist so I haven’t tended to come into contact with patients who my work has helped. But it’s such a privilege when I have. One lady I met a few years ago stays in my mind. Her ovarian cancer had returned and she was offered olaparib as part of a trial. She described how frightening it was to be trying something so new but felt it was her only hope. The drug worked and when we met, she had no signs of the cancer.
She said that I’d given her life back to her. I don’t tend to think of myself as a lifesaver but it’s probably no surprise that I consider the development of olaparib as the most meaningful outcome in my career so far.
When I started out as an independent group leader in Cambridge, nearly everything my group touched seemed to turn to gold. And then a reviewer’s comment made me stop and think. I had brilliant people in my lab at the Gurdon Institute, where I was based when I moved to Cambridge in 1991. We were working in new areas, studying how genes are transcribed into RNA to make proteins and we also had first insights into other cellular processes. We had a brilliant review from our funders at the end of the first five years, but one of the comments questioned whether it was relevant for cancer patients.
I was concerned that great research on its own might not be fundable. We needed to find translational opportunities that would potentially benefit patients.
Meanwhile I’d stumbled across something new and interesting: an enzyme that was activated by breaks in DNA. It took a little time for the penny to drop but, when it did, I realised that something activated by broken DNA is probably involved in DNA repair. The enzyme was part of a ‘molecular police force’ that patrols, spots damage and triggers the fixing processes.
“My Eureka moments?
A counterintuitive idea and a late-night conversation in a bar.”
This started cogs whirring in my brain. I knew that radiation and chemotherapies kill cancer cells by generating DNA damage. Could we make drugs that stop the molecular police from repairing the damage?
I couldn’t get people to buy into the idea… why would you want to inhibit DNA repair? We needDNA repair. It was counterintuitive to think about knocking it out.
One of the great things about Cambridge is that there are lots of examples of very successful biotech start-ups. I thought, if they can do it, why can’t I? And that’s the story of KuDOS, the company I set up in 1997. I was a young professor in Cambridge and the science was new, but a small set of venture capital groups had the confidence to back me in my ideas. Crucially I also had the support of my funders (the predecessors of Cancer Research UK) and the Tech Transfer Office (now Cambridge Enterprise).
The game plan was to go all-out and develop drugs against DNA repair enzymes, including against a protein family called poly ADP-ribose polymerase (PARP) which we knew helped repair broken DNA. Out of this programme came olaparib, a potent PARP inhibitor.
“There’s something about the environment here in Cambridge that not only creates great science. It also really nurtures people and connections.”
And then came the second Eureka moment. I was at a conference in a late night bar talking to Professor Alan Ashworth who at the time was at the Institute for Cancer Research in London. He was working on cells with mutations in genes called BRCA1 and BRCA2, which commonly occur in people with cancer.
DNA repair is so important to our survival that we have evolved a backup mechanism in case PARP fails. One such process is called homologous recombination and it involves DNA being exchanged between identical pieces of DNA to repair it.
Alan and others had figured out that BRCA1 and BRCA2 are very important for homologous recombination. We speculated that if you block the PARP repair mechanism in people with cancers caused by BRCA1/2 defects, their healthy cells might revert to their backup and survive but, because the tumour cells have no BRCA1 or 2, they may have no backup and so would die. This is exactly what scientists in our groups found.
This was the answer. It meant that the PARP inhibitors that KuDOS had developed could be used to treat patients who had BRCA1/2-mutated cancers. Sure enough, when we tested this, the BRCA-deficient cells dropped dead when you gave them a PARP inhibitor at concentrations where normal cells just shrugged their shoulders and carried on growing and dividing.
We published our work in the journal Nature in 2005. It took us almost 18 months to get it through the reviewers. It wasn’t that they didn’t believe it. They were saying – at least for a while – was this really all that exciting and interesting?
Meanwhile, work was moving fast at KuDOS. Olaparib had already gone into healthy volunteers. The next stages of clinical trials were going to be very expensive. The best way forward would be either to partner with a pharmaceutical company to share the risk and share the benefit, or to be acquired by a pharma company, which is what we did. AstraZeneca bought KuDOS in 2006 for $210m.
“I consider olaparib as the most meaningful outcome in my career so far.”
This year marks 10 years since the European Commission granted approval for olaparib, marketed as Lynparza (the trade-name of olaparib) by AstraZeneca, to treat ovarian cancer patients who have BRCA1 or BRCA2 mutations. The drug has been jointly developed and commercialised by AstraZeneca and MSD, and is now approved in several countries across multiple tumour types including forms of breast cancer, pancreatic cancer and prostate cancer.
Then, in 2023,the NHS agreed a deal to roll-out the drug to treat advanced prostate cancer and a form of early breast cancer.
I’m now based at the Cancer Research UK (CRUK) Cambridge Institute, which is next door both to AstraZeneca’s European headquarters and Addenbrooke’s Hospital on the Cambridge Biomedical Campus. I pass clinicians in the Institute corridor who prescribe olaparib for their patients. It’s nearly 35 years since I set up my lab in Cambridge and I oscillate between thinking the time has gone in a flash to thinking it’s been a long slog which nearly did me in!
One thing I’ve learned is that ideas need people to drive them over lines. In particular my KuDOS colleagues Niall Martin, Graeme Smith, Keith Menear and Barrie Ward, as well as Mark O’Connor who brought huge continuity to the drug’s development when he moved to AstraZeneca from KuDOS when it was acquired, and Susan Galbraith at AstraZeneca who had the insight and gravitas to allow the programme to progress. There’s something about the environment here in Cambridge that not only creates great science. It also really nurtures people and connections.
Curiosity is also hugely important. There are a great many things we don’t know and many things we don’t even know we don’t know. The possibility of scientific discovery is what gets me out of bed in the morning.
Science is moving ever more quickly now. I’m hopeful that more of these kinds of drugs will find their way to the right patients in combinations that could be curative for some. Right now, PARP inhibitors are fairly expensive but when they fall off their patent cliff, maybe usage could go from hundreds of thousands to millions of people.
In my view, the future of cancer will also increasingly involve early diagnosis. It’s intriguing to think that, for some patients, it might be possible to take olaparib or other drugs as a preventative treatment to wipe out rogue cells before they even get a chance to become a fully grown cancer.
What’s my advice for early career researchers? Take calculated risks. It’s a shots-on-goal thing: think about the approach, understand the biology, stay curious, and when things do not work out, try again and try something different.
Professor Sir Steve Jackson works at the Cancer Research UK Cambridge Institute. His work has been funded by Cancer Research UK, Wellcome, European Union, European Research Council, Worldwide Cancer Research, the Mark Foundation for Cancer Research and other organisations.
Published:
With thanks to Jackie van Bochoven Words: Louise Walsh Photography: StillVision
Academics and staff from the University of Cambridge are featured in the King’s Birthday Honours 2024, which recognises the achievements and service of people across the UK, from all walks of life.
Professor Tony Kouzarides, Professor of Cancer Biology, Senior Group Leader at the Gurdon Institute and Director and Co-Founder of the Milner Institute, has been awarded a Knighthood for his services to Healthcare Innovation and Delivery. Professor Kouzarides said:“I am delighted to receive this honour, which reinforces the importance of translating basic research into therapies by engaging academic researchers with healthcare businesses.”
Professor Barbara Sahakian, Professor of Clinical Neuropsychology in the Department of Psychiatry and a Fellow at Clare Hall, receives a CBE. Professor Sahakian, who is known for her research aimed at understanding the neural basis of cognitive, emotional and behavioural dysfunction in order to develop more effective pharmacological and psychological treatments, is honoured for her services to Research in Human Cognitive Processes. Professor Sahakian said:“I am delighted to receive this prestigious award, which recognises my research on human cognitive processes in health, psychiatric disorders and neurological diseases. I am grateful to my PhD students, postdoctoral fellows and colleagues for their collaboration.”
Professor Christine Holt, Professor of Developmental Neuroscience, receives a CBE for services to Neuroscience. Professor Holt said: “I’m surprised and thrilled to receive this honour. It’s a marvellous recognition of the research that has involved a whole team of talented, dedicated and inspiring colleagues over many years.”
Professor David Menon, founder of the Neurosciences Critical Care Unit (NCCU) at Addenbrooke’s Hospital, has been awarded a CBE. Professor Menon, who is noted for his national and global clinical and research leadership in traumatic brain injury, is honoured for his services to Neurocritical Care. He said: “I am deeply honoured to be nominated for a CBE and accept it on behalf of all those who have worked with me, during what has been – and continues to be – a very rewarding career.”
Professor Patrick Maxwell, Regius Professor of Physic and Head of School of Clinical Medicine, receives a CBE for services to Medical Research.
Professor Peter John Clarkson, Director of Cambridge Engineering Design Centre and Co-Director of Cambridge Public Health, receives a CBE. Professor Clarkson, who is known for his research in health and care improvement, inclusive design and systems design, is honoured for his services to Engineering and Design. Professor Clarkson said “I am delighted to receive this honour and thank all those extraordinary people I have had the pleasure to work with over the years who have supported me in so many interesting and transformative projects.”
Alexandra Bolton, Director of the Climate Governance Initiative, is awarded an OBE for services to the Built and Natural Environment. Alexandra said: “This wonderful and humbling recognition makes me in turn recognise the talented people who, throughout my career, have selflessly given me support, guidance and advice. I am enormously grateful for the honour, and for all those who have helped me along the way.”
Professor Anne-Christine Davis, Professor of Mathematical Physics, receives an OBE for services to Higher Education and to Scientific Research. Professor Davis said: “I am amazed and overwhelmed to receive this honour. I could not have done it alone and wish to thank my wonderful students and collaborators over the years. I would like to dedicate this honour to those women in STEMM who came before me and did not receive the recognition they deserved.”
Professor Shruti Kapila, Professor of History and Politics receives an OBE for services to Research in Humanities.
Details of University alumni who are recognised in the King’s Birthday Honours will be published on www.alumni.cam.ac.uk.
The University extends its congratulations to all academics, staff and alumni who have received an honour.
Video footage of Iceland’s 2010 Eyjafjallajökull eruption is providing researchers from the University of Cambridge with rare, up-close observations of volcanic ash clouds — information that could help better forecast how far explosive eruptions disperse their hazardous ash particles.
When Eyjafjallajökull erupted in 2010, it ejected roughly 250 million tonnes of volcanic ash into the atmosphere: much of which was blown over Europe and into flight paths. With planes grounded, millions of air passengers were left stranded.
Forecasts of how ash will spread in the aftermath of an explosive eruption can help reduce impacts to aviation by informing decisions to shut down areas of airspace. But these forecasts require knowledge of what is happening at the volcano, information that often can’t be obtained directly and must instead be estimated.
In the new study, the researchers split a 17-minute film into time segments to understand how the Eyjafjallajökull ash cloud grew upwards and outwards as the eruption ensued.
“No one has previously observed the shape and speed of wind-blown ash clouds directly,” said Professor Andy Woods, lead author of the study from Cambridge’s Department of Earth Sciences and Institute for Energy and Environmental Flows. Their new video analysis method was reported in Nature Communications Earth and Environment.
By comparing characteristics of the ash cloud, such as its shape and speed, at time intervals through the video, the researchers were able to calculate the amount of ash spewed from the volcano.
That rate of ash flow, called eruption rate, is an important metric for forecasting ash cloud extent, said Woods. “The eruption rate determines how much ash goes up into the atmosphere, how high the ash cloud will go, how long the plume will stay buoyant, how quickly the ash will start falling to the ground and the area over which ash will land.”
Generally, the higher the ash plume, the wider the ash will be dispersed, and the smaller the ash particles are, the longer they stay buoyant. This dispersal can also depend on weather conditions, particularly the wind direction.
Volcanoes across the world are increasingly monitored via video, using webcams or high-resolution cameras. Woods thinks that, if high frame rate video observations can be accessed during an eruption, then this real-time information could be fed into ash cloud forecasts that more realistically reflect changing eruption conditions.
During the 17-minute footage of the Eyjafjallajökull eruption, the researchers observed that the eruption rate dropped by about half. “It’s amazing that you can learn eruption rate from a video, that’s something that we’ve previously only been able to calculate after an eruption has happened,” said Woods. “It’s important to know the changing eruption rate because that could impact the ash cloud dispersal downwind.”
It’s usually challenging for volcanologists to take continuous measurements of ash clouds whilst an eruption is happening. “Instead, much of our understanding of how ash clouds spread in the atmosphere is based on scaled-down lab models,” said Dr Nicola Mingotti, a researcher in Woods’ group and co-author of this study. These experiments are performed in water tanks, by releasing particle-laden or dyed saline solutions and analysing footage of the plume as it dissipates.
Woods and his collaborators have been running lab experiments like these for several years, most recently trying to understand how eruption plumes are dragged along by the wind. But it’s a big bonus to have video measurements from a real eruption, said Woods, and the real observations agree closely with what they’ve been observing in the lab. “Demonstrating our lab experiments are realistic is really important, both for making sure we understand how ash plumes work and that we forecast their movements effectively.”
Study uncovers how the brain simulates possible future actions by drawing from our stored memories.
In pausing to think before making an important decision, we may imagine the potential outcomes of different choices we could make. While this ‘mental simulation’ is central to how we plan and make decisions in everyday life, how the brain works to accomplish this is not well understood.
An international team of scientists has now uncovered neural mechanisms used in planning. Their results, published in the journal Nature Neuroscience, suggest that an interplay between the brain’s prefrontal cortex and hippocampus allows us to imagine future outcomes to guide our decisions.
“The prefrontal cortex acts as a ‘simulator,’ mentally testing out possible actions using a cognitive map stored in the hippocampus,” said co-author Marcelo Mattar from New York University. “This research sheds light on the neural and cognitive mechanisms of planning—a core component of human and animal intelligence. A deeper understanding of these brain mechanisms could ultimately improve the treatment of disorders affecting decision-making abilities.”
The roles of both the prefrontal cortex—used in planning and decision-making—and hippocampus—used in memory formation and storage—have long been established. However, their specific duties in deliberative decision-making, which are the types of decisions that require us to think before acting, are less clear.
To illuminate the neural mechanisms of planning, Mattar and his colleagues—Kristopher Jensen from University College London and Professor Guillaume Hennequin from Cambridge’s Department of Engineering —developed a computational model to predict brain activity during planning. They then analysed data from both humans and rats to confirm the validity of the model—a recurrent neural network (RNN), which learns patterns based on incoming information.
The model took into account existing knowledge of planning and added new layers of complexity, including ‘imagined actions,’ thereby capturing how decision-making involves weighing the impact of potential choices—similar to how a chess player envisions sequences of moves before committing to one. These mental simulations of potential futures, modelled as interactions between the prefrontal cortex and hippocampus, enable us to rapidly adapt to new environments, such as taking a detour after finding a road is blocked.
The scientists validated this computational model using both behavioural and neural data. To assess the model’s ability to predict behaviour, the scientists conducted an experiment measuring how humans navigated an online maze on a computer screen and how long they had to think before each step.
To validate the model’s predictions about the role of the hippocampus in planning, they analysed neural recordings from rodents navigating a physical maze configured in the same way as in the human experiment. By giving a similar task to humans and rats, the researchers could draw parallels between the behavioural and neural data—an innovative aspect of this research.
“Allowing neural networks to decide for themselves when to ‘pause and think’ was a great idea, and it was surprising to see that in situations where humans spend time pondering what to do next, so do these neural networks,” said Hennequin.
The experimental results were consistent with the computational model, showing an intricate interaction between the prefrontal cortex and hippocampus. In the human experiments, participants’ brain activity reflected more time thinking before acting in navigating the maze. In the experiments with laboratory rats, the animals’ neural responses in moving through the maze resembled the model’s simulations.
“Overall, this work provides foundational knowledge on how these brain circuits enable us to think before we act in order to make better decisions,” said Mattar. “In addition, a method in which both human and animal experimental participants and RNNs were all trained to perform the same task offers an innovative and foundational way to gain insights into behaviours.”
“This new framework will enable systematic studies of thinking at the neural level,” said Hennequin. “This will require a concerted effort from neurophysiologists and theorists, and I’m excited about the discoveries that lie ahead.”
Astronomers have detected carbon in a galaxy just 350 million years after the Big Bang, the earliest detection of any element in the universe other than hydrogen.
Using the James Webb Space Telescope (JWST), an international team of astronomers led by the University of Cambridge observed a very young galaxy in the early universe and found that it contained surprising amounts of carbon, one of the seeds of life as we know it.
In astronomy, elements heavier than hydrogen or helium are classed as metals. The very early universe was almost entirely made up of hydrogen, the simplest of the elements, with small amounts of helium and tiny amounts of lithium.
Every other element that makes up the universe we observe today was formed inside a star. When stars explode as supernovas, the elements they produce are circulated throughout their host galaxy, seeding the next generation of stars. With every new generation of stars and ‘stardust’, more metals are formed, and after billions of years, the universe evolves to a point where it can support rocky planets like Earth and life like us.
The ability to trace the origin and evolution of metals will help us understand how we went from a universe made almost entirely of just two chemical elements, to the incredible complexity we see today.
“The very first stars are the holy grail of chemical evolution,” said lead author Dr Francesco D’Eugenio, from the Kavli Institute for Cosmology at Cambridge. “Since they are made only of primordial elements, they behave very differently to modern stars. By studying how and when the first metals formed inside stars, we can set a time frame for the earliest steps on the path that led to the formation of life.”
Carbon is a fundamental element in the evolution of the universe, since it can form into grains of dust that clump together, eventually forming into the first planetesimals and the earliest planets. Carbon is also key for the formation of life on Earth.
“Earlier research suggested that carbon started to form in large quantities relatively late – about one billion years after the Big Bang,” said co-author Professor Roberto Maiolino, also from the Kavli Institute. “But we’ve found that carbon formed much earlier – it might even be the oldest metal of all.”
The team used the JWST to observe a very distant galaxy – one of the most distant galaxies yet observed – just 350 million years after the Big Bang, more than 13 billion years ago. This galaxy is compact and low mass – about 100,000 times less massive than the Milky Way.
“It’s just an embryo of a galaxy when we observe it, but it could evolve into something quite big, about the size of the Milky Way,” said D’Eugenio. “But for such a young galaxy, it’s fairly massive.”
The researchers used Webb’s Near Infrared Spectrograph (NIRSpec) to break down the light coming from the young galaxy into a spectrum of colours. Different elements leave different chemical fingerprints in the galaxy’s spectrum, allowing the team to determine its chemical composition. Analysis of this spectrum showed a confident detection of carbon, and tentative detections of oxygen and neon, although further observations will be required to confirm the presence of these other elements.
“We were surprised to see carbon so early in the universe, since it was thought that the earliest stars produced much more oxygen than carbon,” said Maiolino. “We had thought that carbon was enriched much later, through entirely different processes, but the fact that it appears so early tells us that the very first stars may have operated very differently.”
According to some models, when the earliest stars exploded as supernovas, they may have released less energy than initially expected. In this case, carbon, which was in the stars’ outer shell and was less gravitationally bound than oxygen, could have escaped more easily and spread throughout the galaxy, while a large amount of oxygen fell back and collapsed into a black hole.
“These observations tell us that carbon can be enriched quickly in the early universe,” said D’Eugenio. “And because carbon is fundamental to life as we know it, it’s not necessarily true that life must have evolved much later in the universe. Perhaps life emerged much earlier – although if there’s life elsewhere in the universe, it might have evolved very differently than it did here on Earth.”
The research was supported in part by the European Research Council, the Royal Society, and the Science and Technology Facilities Council (STFC), part of UK Research and Innovation (UKRI).
Reference: Francesco D’Eugenio et al. ‘JADES: Carbon enrichment 350 Myr after the Big Bang.’ Astronomy & Astrophysics (in press). DOI: 10.48550/arXiv.2311.09908
Assumptions that tropical forest canopies protect from the effects of climate change are unfounded, say researchers.
A severe risk is that species are no longer able to survive within tropical forests as climate change intensifies, further exacerbating the global extinction crisis and degrading rainforest carbon stocks.David Edwards
Crucial strongholds for biodiversity are under threat as temperatures are rising in tropical forests, the world’s most diverse terrestrial ecosystems, a new study reveals.
It has been long assumed that the forest subcanopy and understorey – where direct sunlight is reduced – would be insulated from the worst climate change impacts by the shielding effect of the forest canopy.
This showed that between 2005 and 2019, most of the world’s undisturbed tropical forests experienced climate conditions at least partially outside the range of historic conditions. Many areas had transitioned to almost entirely new temperature averages.
Until recently, temperatures beneath the canopy in rainforests have remained relatively stable, meaning that the wildlife that lives there has evolved within a narrow range of temperatures. This leaves it poorly adapted to deal with temperatures outside this range.
The study found pronounced shifts in climate regimes in a significant proportion of tropical forests, including globally important national parks, indigenous reserves, and large tracts of ecologically unfragmented areas.
Recent studies in largely undisturbed, or primary lowland tropical forests have found changes in species composition and significant declines in animal, insect, and plant populations. These changes are attributed to warming temperatures and are consistent with the findings of the new research.
“Tropical forests are the true powerhouses of global biodiversity, and the complex networks of species they contain underpin vast carbon stocks that help to mitigate climate change. A severe risk is that species are no longer able to survive within tropical forests as climate change intensifies, further exacerbating the global extinction crisis and degrading rainforest carbon stocks,” said Professor David Edwards at the University of Cambridge’s Department of Plant Sciences, a study co-author.
“Our study challenges the prevailing notion that tropical forest canopies will mitigate climate change impacts and it helps us understand how to prioritise conservation of these key areas of biodiversity effectively,” said Dr Alexander Lees, Reader in Biodiversity at Manchester Metropolitan University, a study co-author.
He added: “It is paramount that distant, wealth-related drivers of deforestation and degradation are addressed and that the future of those forests acting as climate refuges is secured by effecting legal protection, and by empowering indigenous communities.
“Notwithstanding the fundamental need for global carbon emission reductions, the prioritisation and protection of refugia and the restoration of highly threatened forests is vital to mitigate further damage to global tropical forest ecosystems.”
“Tropical forests, home to many of the world’s highly specialised species, are particularly sensitive to even small changes in climate,” said Dr Brittany Trew, Conservation Scientist for the Royal Society for the Protection of Birds, and lead author of the study.
She added: “Our research shows that climate change is already impacting vast areas of pristine tropical forest globally. To provide species with the best chance to adapt to these changes, these forests must be protected from additional human-induced threats.”
“The world’s rainforests are incredible reservoirs of biodiversity, harbouring species that live in micro-environments in which climate conditions are generally stable. Thus, they are particularly sensitive to any changes brought about by climate change. It is vital that we take measures to safeguard these ecosystems from human pressures,” said Ilya Maclean, Professor of Global Change Biology at the University of Exeter and senior author of the study.
The study was made possible through a global collaboration that included researchers at Mountains of the Moon University, Uganda; Universidade Federal do Pará, Brazil; the Brazilian Agricultural Research Corporation and Universidad Nacional de San Antonio Abad del Cusco, Perú. It was funded by the National Science Foundation (NSF).
Two decades of cuckoo research have helped scientists to explain how battles between species can cause new species to arise
This exciting new finding could potentially apply to any pairs of species that are in battle with each other…the coevolutionary arms race could cause new species to emerge – and increase biodiversity on our planetRebecca Kilner
The theory of coevolution says that when closely interacting species drive evolutionary changes in each other this can lead to speciation – the evolution of new species. But until now, real-world evidence for this has been scarce.
Now a team of researchers has found evidence that coevolution is linked to speciation by studying the evolutionary arms race between cuckoos and the host birds they exploit.
Bronze-cuckoos lay their eggs in the nests of small songbirds. Soon after the cuckoo chick hatches, it pushes the host’s eggs out of the nest. The host not only loses all its own eggs, but spends several weeks rearing the cuckoo, which takes up valuable time when it could be breeding itself.
Each species of bronze-cuckoo closely matches the appearance of their host’s chicks, fooling the host parents into accepting the cuckoo.
The study shows how these interactions can cause new species to arise when a cuckoo species exploits several different hosts. If chicks of each host species have a distinct appearance, and hosts reject odd-looking nestlings, then the cuckoo species diverges into separate genetic lineages, each mimicking the chicks of its favoured host. These new lineages are the first sign of new species emerging.
“This exciting new finding could potentially apply to any pairs of species that are in battle with each other. Just as we’ve seen with the cuckoo, the coevolutionary arms race could cause new species to emerge – and increase biodiversity on our planet,” said Professor Kilner in the University of Cambridge’s Department of Zoology, a co-author of the report.
The striking differences between the chicks of different bronze-cuckoo lineages correspond to subtle differences in the plumage and calls of the adults, which help males and females that specialise on the same host to recognise and pair with each other.
“Cuckoos are very costly to their hosts, so hosts have evolved the ability to recognise and eject cuckoo chicks from their nests,’’ said Professor Naomi Langmore at the Australian National University, Canberra, lead author of the study.
She added: “Only the cuckoos that most resemble the host’s own chicks have any chance of escaping detection, so over many generations the cuckoo chicks have evolved to mimic the host chicks.”
The study revealed that coevolution is most likely to drive speciation when the cuckoos are very costly to their hosts, leading to a ‘coevolutionary arms race’ between host defences and cuckoo counter-adaptations.
A broad scale analysis across all cuckoo species found that those lineages that are most costly to their hosts have higher speciation rates than less costly cuckoo species and their non-parasitic relatives.
“This finding is significant in evolutionary biology, showing that coevolution between interacting species increases biodiversity by driving speciation,” said Dr Clare Holleley at the Australian National Wildlife Collection within CSIRO, Canberra, senior author of the report.
The study was made possible by the team’s breakthrough in extracting DNA from eggshells in historical collections, and sequencing it for genetic studies.
The researchers were then able to combine two decades of behavioural fieldwork with DNA analysis of specimens of eggs and birds held in museums and collections.
The study involved an international team of researchers at the University of Cambridge, Australian National University, CSIRO (Australia’s national science agency), and the University of Melbourne. It was funded by the Australian Research Council.





 and patient at two days (centre) and six weeks (right) after severe traumatic brain injury (Credit: Virginia Newcombe)")